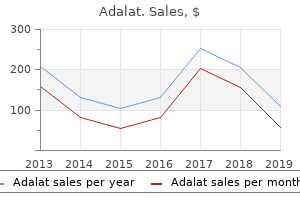
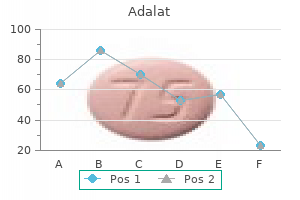
Adalat
David F. M. Brown, M.D. - Instructor in Medicine
- Harvard Medical School
- Massachusetts General Hospital
- Boston, MA
Safe 20mg adalatMoreover arrhythmia zoloft generic adalat 30 mg line, the absence of reflex will increase in heart rate can make patients particularly delicate to speedy vasodilation heart attack or pulled muscle 30mg adalat with mastercard. Isoproterenol or epinephrine infusions must be available to increase the guts price if needed adderall xr hypertension cheap adalat 20 mg. Direct arterial pressure monitoring ought to be used for main operations; strict asepsis ought to be noticed during placement prehypertension discount 30 mg adalat overnight delivery. In a lately transplanted affected person, the best ventricle of the transplanted coronary heart might not be able to overcome the resistance of the pulmonary vasculature. Right ventricular failure can happen perioperatively, requiring the use of inhaled nitric oxide, inotropes, and, at occasions, right ventricular help gadgets. Maintenance of proper heart perform is essential to adequately provide the left facet of the guts with adequate blood for the device to eject. A history of syncope in elderly patients should always raise the potential of arrhythmias and underlying organic heart illness. Although arrhythmias can occur within the absence of natural heart illness, the two are commonly associated. Cardiac syncope usually results from an abrupt arrhythmia that suddenly compromises cardiac output and impairs cerebral perfusion. Lightheadedness and presyncope, could replicate lesser levels of cerebral impairment. Reversible abnormalities may be as a result of abnormal vagal tone, electrolyte abnormalities, drug toxicity, hypothermia, or myocardial ischemia. Irreversible abnormalities, which initially could additionally be solely intermittent before they become permanent, reflect both isolated conduction system abnormalities or underlying coronary heart disease (most commonly hypertensive, coronary artery, or valvular coronary heart disease). She provides a historical past of two episodes of lightheadedness a number of days prior to her fall at present. The significance of a conduction system abnormality is dependent upon its location, its likelihood for progression to full coronary heart block, and the chance that a more distal pacemaker website will be in a position to maintain a steady and enough escape rhythm (>40 beats/min). The His bundle is generally the lowest space in the conduction system that may maintain a stable rhythm (usually 40�60 beats/min). What is the significance of isolated bundlebranch block with a traditional P�R interval The time period hemiblock is usually used if solely one of the two fascicles of the left bundle-branch is blocked (left anterior or left posterior hemiblock). When the P�R interval is normal-and within the absence of an acute (>3 s) or the effective ventricular price is less than 40 beats/min. Patients might expertise intermittent dizziness, syncope, confusion, fatigue, or shortness of breath. The time period tachycardia�bradycardia syndrome is often used when sufferers expertise paroxysmal tachyarrhythmias (usually atrial flutter or fibrillation) followed by sinus pauses or bradycardia. During isorhythmic dissociation, the atria and ventricles beat independently at practically the same price. A bifascicular block exists when two of the three major His bundle-branches (right, left anterior, or left posterior) are partially or utterly blocked. Intracardiac electrocardiographic recordings would be essential to affirm the site of the conduction delay. One of two approaches may be recommended, depending on the urgency of the surgery. If the surgery is actually emergent, a quick lived transvenous pacing catheter or a transcutaneous pacemaker is indicated previous to induction of general or regional anesthesia. The first three indications generally require ventricular pacing, whereas the fourth requires atrial pacing electrodes and a programmable rapid atrial pulse generator. Pacing may be established by transvenous, transcutaneous, epicardial, or transesophageal electrodes. The most reliable methodology is usually through a transvenous pacing electrode within the type of a pacing wire or a balloon-tipped pacing catheter. A pacing wire should always be positioned fluoroscopically, but a flow-directed pacing catheter can additionally be positioned in the best ventricle beneath pressure monitoring. Once positioned, the pacing electrodes are hooked up to an electrical pulse generator that periodically delivers an impulse at a set fee and magnitude. The lowest present through the electrode that can depolarize the myocardium is known as the threshold current (usually <2 mA for transvenous electrodes). Ventricular pacing typically reduces cardiac output as a end result of the atrial contribution to ventricular filling is misplaced. The P�R interval could be diversified by adjusting the delay between the atrial and ventricular impulses (usually set at 150�200 ms). Pacemakers are categorized by a five-letter code, based on the chambers paced, chambers sensed, response to sensing, programmability, and arrhythmia perform (Table 21�20). The spike price must be identical to the programmed (permanent pacemaker-usually 72/min) or set (temporary) pacemaker rate; a slower price might indicate a low battery. If the affected person has a brief pacemaker, the escape rhythm could be established by temporarily slowing the pacing rate. Chamber Paced O = none A = atrium V = ventricle D = dual (atrium and ventricle) Chamber Sensed O = none A = atrium V = ventricle D = dual (atrium and ventricle) Response to Sensing O = none T = triggered l = inhibited D = twin (triggered and inhibited) Programmability O = none P = easy M = multiprogrammable C = communicating R = price modulation Antitachyarrhythmia Function O = none P = pacing S = shock D = dual (pacing and shock) What intraoperative situations might trigger the pacemaker to malfunction Electrical interference from surgical electrocautery items may be interpreted as myocardial electrical activity and can suppress the pacemaker generator. Problems with electrocautery may be minimized by limiting its use to short bursts, limiting its power output, inserting its grounding plate as removed from the pacemaker generator as possible, and using bipolar cautery. Moreover, continuous monitoring of an arterial pulse wave (pressure, plethysmogram, or oximetry signal) is obligatory to guarantee steady perfusion during electrocautery. If a temporary pacemaker fails intraoperatively, the inspired oxygen focus must be increased to 100%. Most items have a battery-level indicator and a light that flashes with each impulse. The generator must be set into the asynchronous mode, and the ventricular output must be set on most. Failure of a temporary transvenous electrode to seize the ventricle is normally as a outcome of displacement of the electrode away from the ventricular endocardium; careful slow advancement of the catheter or wire while pacing often leads to seize. Pharmacological administration (atropine, isoproterenol, or epinephrine) may be useful till the issue is resolved. If a everlasting pacemaker malfunctions (as with electrocautery), it ought to usually be transformed to an asynchronous mode. Some units will mechanically reprogram themselves to the asynchronous mode if malfunction is detected. Other pacemaker units have to be reprogrammed by placing either an exterior magnet, or, preferably, a programming gadget over the generator. The effect of an external magnet on some pacemakers-particularly during electrocautery-may be unpredictable and will usually be decided prior to surgery. All anesthetic brokers have been safely used in sufferers who have already got pacemakers.
Diseases - Myelinopathy
- Adie syndrome
- Chen-Kung Ho Kaufman Mcalister syndrome
- Leao Ribeiro Da Silva syndrome
- Mental retardation progressive spasticity
- Achondroplasia Swiss type agammaglobulinemia
- Drachtman Weinblatt Sitarz syndrome
- Congenital toxoplasmosis
- Portal vein thrombosis
- Cardiomyopathic lentiginosis
Adalat: 30 mg, 20 mg
Adalat 20mg lineAssisted and controlled air flow require positive stress during inspiration to broaden the lungs blood pressure kit cvs buy cheap adalat 20 mg. Performance Characteristics of Mapleson Circuits Mapleson circuits are light-weight hypertension lifestyle changes cheap adalat 20 mg amex, inexpensive blood pressure medication that does not cause joint pain generic 30 mg adalat with visa, and simple pulmonary hypertension zebra purchase adalat 20 mg without prescription. Because a recent gas circulate equal to minute air flow is adequate to stop rebreathing, the Mapleson A design is probably the most efficient Mapleson circuit for spontaneous air flow. Although some alveolar and fresh fuel exits via the valve during inspiration, no fuel is vented during expiration, because the exhaled gasoline stagnates during the expiratory section of positive-pressure ventilation. As a outcome, very high recent gas flows (greater than 3 times minute ventilation) are required to stop rebreathing with a Mapleson A circuit throughout managed air flow. Thus, simply transferring components utterly alters the fresh fuel necessities of the Mapleson circuits. A drawback of this coaxial circuit is the risk of kinking or disconnection of the contemporary fuel inlet tubing. Periodic inspection of the inner tubing is necessary to determine this complication; if unrecognized, both of these mishaps could end in important rebreathing of exhaled gas. Carbon Dioxide Absorber and the Absorbent Rebreathing alveolar gasoline conserves warmth and humidity. In an attempt to avoid these problems, the circle system provides more components to the respiration system. Reaction end products embody heat (the warmth of neutralization), water, and calcium carbonate. It consists primarily of calcium hydroxide (80%), along with sodium hydroxide, water, and a small amount of potassium hydroxide. Another absorbent, barium hydroxide lime, is now not used because of the attainable elevated hazard of fireplace in the respiratory system. A pH indicator dye (eg, ethyl violet) adjustments color from white to purple as a consequence of increasing hydrogen ion concentration and absorbent exhaustion. Although exhausted granules might revert to their authentic colour if rested, no important restoration of absorptive capability occurs. Granule dimension is a compromise between the higher absorptive surface space of small granules and the decrease resistance to gasoline circulate of bigger granules. Increasing the hardness of soda lime by adding silica minimizes the risk of inhalation of sodium hydroxide mud and likewise decreases resistance of gas flow. Additional water is added to absorbent during packaging to present optimum circumstances for carbonic acid formation. Volatile anesthetics may be damaged all the way down to carbon monoxide by dry absorbent (eg, sodium or potassium hydroxide) sufficiently to cause clinically measureable carboxyhemoglobin concentrations. The formation of carbon monoxide is best with desflurane; with sevoflurane, it occurs at the next temperature. It possesses larger inertness than soda lime, leading to much less degradation of risky anesthetics (eg, sevoflurane into compound A or desflurane into carbon monoxide). Higher concentrations of sevoflurane, extended publicity, and low-flow anesthetic approach seem to increase the formation of compound A. Compound A has been proven to produce nephrotoxicity in animals but has never been related to ill results in people. The granules of absorbent are contained within one or two canisters that fit snugly between a head and base plate. Channeling through areas of loosely packed granules is minimized by a baffle system, which directs fuel flow through the center, thereby permitting larger utilization of the absorbent. Forward move displaces the disk upward, permitting the gasoline to proceed via the circuit. Condensation and resultant moisture formation might prevent upward displacement of the disks, resulting in incomplete escape of expired gases and rebreathing. The subsequent flow of fuel away from the patient throughout exhalation opens the expiratory valve. Closure of the inspiratory valve throughout exhalation prevents expiratory gasoline from mixing with 7 recent gasoline in the inspiratory limb. Positioning it downstream from the inspiratory valve would allow contemporary gasoline to bypass the affected person during exhalation and be wasted. Fresh fuel introduced between the expiratory valve and the absorber can be diluted by recirculating gas. Furthermore, inhalation anesthetics may be absorbed or launched by soda lime granules, thus slowing induction and emergence. The latter is a mixture of fresh gasoline and exhaled fuel that has passed by way of the absorber. Higher flows speed induction and restoration, compensate for leaks in the circuit, and reduce the risks of unanticipated gas mixtures. Bacterial Contamination the minimal danger of microorganism retention in circle system parts may theoretically result in respiratory infections in subsequent patients. For this purpose, bacterial filters are generally included into the inspiratory or expiratory breathing tubes or at the Y-piece. Disadvantages of the Circle System Although most of the issues of Mapleson circuits are solved by the circle system, the improvements have led to different disadvantages: higher size and fewer portability; increased complexity, leading to a better threat of disconnection or malfunction; issues related to use of absorbent; and the difficulty of predicting inspired fuel concentrations throughout low recent gas flows. Thus, any improve in dead area must be accompanied by a corresponding improve in tidal quantity, if 9 alveolar air flow is to remain unchanged. Like Mapleson circuits, length does affect circuit compliance and thus the quantity of tidal volume misplaced to the circuit during positive-pressure ventilation. Pediatric circle techniques might have each a septum dividing the inspiratory and expiratory fuel in the Y-piece and low-compliance respiration tubes to additional scale back lifeless area, and are lighter in weight. Resistance the unidirectional valves and absorber enhance circle system resistance, especially at high respiratory rates and huge tidal volumes. Nonetheless, even untimely neonates may be successfully ventilated using a circle system. Humidity and Heat Conservation Medical fuel supply systems provide dehumidified gases to the anesthesia circuit at room temperature. Therefore, the warmth and humidity of impressed gas depend on the relative proportion of rebreathed fuel to fresh gas. High flows are accompanied by low relative humidity, whereas low flows allow greater water saturation. Absorbent granules present a major supply of heat and moisture in the circle system. A resuscitator is unlike a Mapleson circuit or a circle system as a end result of it accommodates a nonrebreathing valve. The patient valve opens during managed or spontaneous inspiration to permit gas circulate from the air flow bag to the patient. Rebreathing is prevented by venting exhaled gasoline to the atmosphere by way of exhalation ports in this valve. This valve closes throughout bag compression, allowing positive-pressure air flow. The bag is refilled by move by way of the recent fuel inlet and throughout the consumption valve. The reservoir valve meeting is basically two unidirectional valves: the inlet valve and the outlet valve.
Buy adalat 30 mg low priceThey are coated inferiorly and laterally by the bulbospongiosus muscles extending along their length blood pressure grapefruit adalat 20 mg free shipping. The higher vestibular glands are round or oval and are partly overlapped posteriorly by the bulbs of the vestibule blood pressure chart free printable cheap 30mg adalat with amex. The slender ducts of those glands cross deep to the bulbs of the vestibule and open into the vestibule on both sides of the vaginal orifice prehypertension vegetarian buy adalat 20mg low cost. These glands secrete mucus into the vestibule of the vagina throughout sexual arousal (see the Clinical Box "Infection of Greater Vestibular Glands") hypertension in 9th month of pregnancy cheap adalat 30 mg mastercard. The lesser vestibular glands are small glands on all sides of the vestibule of the vagina that open into it between the urethral and vaginal orifices. These glands secrete mucus into the vestibule, which moistens the labia and vestibule. The inner pudendal artery supplies a lot of the pores and skin, exterior genitalia, and perineal muscular tissues. The labial arteries are branches of the internal pudendal artery, as are these of the clitoris. The labial veins are tributaries of the internal pudendal veins and accompanying veins of the internal pudendal artery. Erectile sinus engorgement during the excitement part of the sexual response causes a rise in the measurement and consistency of the clitoris and bulbs of the vestibule of the vagina. The anterior side of the vulva (mons pubis, anterior labia) is equipped by derivatives of the lumbar plexus: the anterior labial nerves, derived from the ilio-inguinal nerve, and the genital branch of the genitofemoral nerve. Its posterior labial nerves (terminal superficial branches of the perineal nerve) provide the labia. Deep and muscular branches of the perineal nerve supply the orifice of the vagina and superficial perineal muscles. The dorsal nerve of the clitoris supplies deep perineal muscle tissue and sensation to the clitoris (see the Clinical Box "Pudendal and Ilio-Inguinal Nerve Blocks"). In this view, the skin, subcutaneous tissue, and ischio-anal fat bodies have been eliminated. Most of the world and most features of the perineum are innervated by branches of the pudendal nerve (S2�S4). The bulb of the vestibule and erectile our bodies of the clitoris obtain parasympathetic fibers through cavernous nerves from the uterovaginal nerve plexus. Parasympathetic stimulation produces elevated vaginal secretion, erection of the clitoris, and engorgement of erectile tissue within the bulbs of the vestibule. Lymph from the skin of the perineum, including the anoderm inferior to the pectinate line of the anorectum and the inferiormost vagina, vaginal orifice, and vestibule, drains initially to the superficial inguinal lymph nodes. The operation, usually performed throughout childhood, removes the prepuce of the clitoris however often additionally removes half or the entire clitoris and labia minora and should embody suturing of the vaginal ostium. This disfiguring procedure is erroneously thought to inhibit sexual arousal and gratification. Vulvar Trauma the mostly vascular bulbs of the vestibule are susceptible to disruption of vessels as the results of trauma. These accidents typically end in severe ache, vulvar hematomas (localized collection of blood) in the labia majora, and scarring and, in some cases, could lead to future obstructed labor or fistula formation. Infection of Greater Vestibular Glands 1521 the larger vestibular glands are usually not palpable however are when contaminated. Occlusion of the vestibular gland duct can predispose the person to an infection of the greater vestibular gland. Bartholinitis, inflammation of the higher vestibular (Bartholin) glands, might end result from a number of pathogenic organisms. Infected glands may enlarge to a diameter of 4�5 cm and impinge on the wall of the rectum. The injection is made where the pudendal 1522 nerve crosses the lateral aspect of the sacrospinous ligament, close to its attachment to the ischial spine or within the initial part of the pudendal canal. To abolish sensation from the anterior part of the perineum, an ilio-inguinal 1523 nerve block is performed. Other forms of anesthesia for childbirth are explained and compared within the Clinical Box "Anesthesia for Childbirth" (earlier in this chapter). Exercises for Strengthening of Female Perineal Muscles the superficial transverse perineal muscle, bulbospongiosus, and exterior anal sphincter, by way of their frequent attachment to the perineal body, type crossing beams over the pelvic outlet to help the perineal body and pelvic diaphragm, as in males. In the absence of the useful calls for associated to urination, penile erection, and ejaculation in males, the muscular tissues are generally relatively underdeveloped in ladies. However, when developed, they contribute to the assist of the pelvic viscera and help stop urinary stress incontinence and postpartum prolapse of pelvic viscera. Therefore, many gynecologists as properly as prepartum classes for participatory childbirth recommend that ladies follow Kegel workout routines (named for A. Some prepartum childbirth classes teach that in studying to voluntarily contract and loosen up the perineal muscular tissues, ladies may be able to resist the tendency to contract the musculature during uterine contractions, permitting a much less obstructed passage for the fetus and decreasing the likelihood of tearing the perineal muscle tissue. Vaginismus Vaginismus is outlined as involuntary (reflex) muscle spasms that occur when vaginal penetration is tried (when perineal muscle tissue are distended). It may trigger dyspareunia (painful intercourse); in extreme 1524 varieties, it prevents vaginal entry. Vaginismus is a physical dysfunction that, for some ladies, has a psychological component, similar to anticipated worry of pain with penetration. For others, vaginismus may be linked to a gynecologic dysfunction, medical situation, or medication. Treatment usually involves muscle relaxation methods and desensitization with using vaginal dilators of accelerating diameter. It contains two elements of the lower limb: the rounded, distinguished posterior area, the buttocks (L. The gluteal area is bounded superiorly by the iliac crest, medially by the intergluteal cleft (natal cleft), and inferiorly by the pores and skin fold (groove) underlying the buttocks, the gluteal fold (L. The gluteal muscles, overlying the pelvic girdle, constitute the bulk of this area. The femoral area (thigh) is the area of the free lower limb that lies between the gluteal, belly, and perineal regions proximally and the knee region distally. The transition from the trunk to the free lower limb happens abruptly within the inguinal region (groin). Here, the boundary between the belly and perineal areas and the femoral region is demarcated by the inguinal ligament anteriorly and the ischiopubic ramus of the hip bone (part of the pelvic girdle or skeleton of the pelvis) medially. Initially, the development of the lower limb is much like that of the upper limb, although occurring a couple of week later. Both limbs initially prolong from the trunk with their creating thumbs and great toes directed superiorly and the palms and soles directed anteriorly. The upper and lower limbs develop from limb buds that arise from the lateral physique wall in the course of the 4th and fifth weeks, respectively. Segmental innervation is maintained, the dermatomal sample reflecting the elongation and spiraling of the limb.
Buy adalat 30mg lineChanging the side-chain structure (R1 blood pressure ratio discount adalat 20mg, R2 arrhythmia questions buy adalat 30 mg cheap, R3) of naturally occurring catecholamines has led to the event of artificial catecholamines (eg blood pressure potassium buy adalat 30 mg low cost, isoproterenol and dobutamine) blood pressure 9040 order 30 mg adalat amex, which are inclined to be extra receptor specific. Adrenergic agonists generally used in anesthesiology are mentioned individually under. Note that the really helpful doses for continuous infusion are expressed as mcg/kg/min for some brokers and mcg/min for others. In both case, these recommendations ought to be regarded solely as guidelines, as particular person responses are fairly variable. The primary impact of phenylephrine is peripheral vasoconstriction with a concomitant rise in systemic vascular resistance and arterial blood strain. The length of action is brief, lasting approximately 15 min after administration of a single dose. Phenylephrine have to be diluted from a 1% solution (10 mg/1-mL ampule), usually to a one hundred mcg/mL solution and titrated to impact. More lately, it and other 2-agonists are increasingly being used for his or her sedative properties. Various research have examined the anesthetic results of oral (3�5 mcg/kg), intramuscular (2 mcg/kg), intravenous (1�3 mcg/kg), transdermal (0. During common anesthesia, clonidine reportedly enhances intraoperative circulatory stability by lowering catecholamine ranges. During regional anesthesia, including peripheral nerve block, clonidine prolongs the period of the block. Direct results on the spinal twine could also be mediated by 2-postsynaptic receptors throughout the dorsal horn. Other potential benefits include decreased postoperative shivering, inhibition of opioid-induced muscle rigidity, attenuation of opioid withdrawal symptoms, and the remedy of acute postoperative ache and a few continual pain syndromes. Side effects embody bradycardia, hypotension, sedation, respiratory melancholy, and dry mouth. Compared with clonidine, dexmedetomidine is more selective for 2-receptors (2:1 specificity ratio is 200:1 for clonidine and 1600:1 for dexmedetomidine). It has sedative, analgesic, and sympatholytic results that blunt many of the cardiovascular responses seen during the perioperative interval. The sedative and analgesic results are mediated by 2adrenergic receptors within the brain (locus ceruleus) and spinal twine. When used intraoperatively, dexmedetomidine reduces intravenous and volatile anesthetic necessities; when used postoperatively, it reduces concurrent analgesic and sedative necessities. Dexmedetomidine is beneficial in sedating patients in preparation for awake fiberoptic intubation. It can additionally be a helpful agent for sedating sufferers postoperatively in postanesthesia and intensive care units, because it does so with out significant ventilatory despair. Rapid administration might elevate blood strain, but hypotension and bradycardia can happen throughout ongoing therapy. The really helpful dosing of dexmedetomidine consists of a loading dose at 1 mcg/kg over 10 min followed by an infusion at 0. Because of the increased affinity of dexmedetomidine for the 2-receptor, in contrast with that of clonidine, this syndrome might manifest after only forty eight h of dexmedetomidine use when the drug is discontinued. Systolic blood stress rises, although 2-mediated vasodilation in skeletal muscle could lower diastolic pressure. Administration of epinephrine is the principal pharmacological therapy for anaphylaxis and can be used to deal with ventricular fibrillation. Complications embody cerebral hemorrhage, myocardial ischemia, and ventricular arrhythmias. Volatile anesthetics, significantly halothane, potentiate the arrhythmic results of epinephrine. In main anaphylactic reactions, epinephrine must be used at a dose of a hundred to 500 mcg (repeated, if necessary) followed by infusion. To enhance myocardial contractility or coronary heart rate, a continuous infusion is ready (1 mg in 250 mL [4 mcg/mL]) and run at a fee of 2 to 20 mcg/min (30�300 ng/kg/min). Epinephrine native infiltration can additionally be used to reduce bleeding from the operative websites. Some local anesthetic options containing epinephrine at a focus of 1:200,000 (5 mcg/mL) or 1:four hundred,000 (2. Epinephrine is available in vials at a concentration of 1:1000 (1 mg/mL) and prefilled syringes at a concentration of 1:10,000 (0. Increased myocardial contractility from 1 results, together with peripheral vasoconstriction, contributes to a rise in arterial blood stress. Both systolic and diastolic pressures usually rise, however increased afterload and reflex bradycardia could forestall any elevation in cardiac output. Decreased renal and splanchnic blood move and elevated myocardial oxygen necessities are concerns, but norepinephrine is the agent of alternative in the management of refractory (particularly septic) shock. Extravasation of norepinephrine on the web site of intravenous administration may cause tissue necrosis. Norepinephrine is administered usually as a steady infusion as a end result of its quick half-life at a fee of 2 to 20 mcg/min (30�300 ng/kg/min). There are important variations, nonetheless: Ephedrine has an extended length of motion, is way much less potent, has both indirect and direct actions, and stimulates the central nervous system (it raises minimum alveolar concentration). The oblique agonist properties of ephedrine may be because of peripheral postsynaptic norepinephrine release or inhibition of norepinephrine reuptake. Currently phenylephrine is extensively utilized in obstetric patients present process neuroaxial anesthesia due its faster onset, shorter length of action, simpler titration, and lack of opposed results on fetal pH relative to ephedrine. When used in moderate doses (3�10 mcg/kg/min), 1 stimulation will increase myocardial contractility, coronary heart price, systolic blood strain, and cardiac output. The 1 effects turn out to be distinguished at larger doses (10�20 mcg/ kg/min), inflicting an increase in peripheral vascular resistance and a fall in renal blood move. The actual dose�response curve for dopamine and these several actions is way more unpredictable than the preceding paragraph would suggest! Systolic blood strain may enhance or remain unchanged, but 2 stimulation decreases peripheral vascular resistance and diastolic blood stress. Myocardial oxygen demand increases while oxygen supply falls, making isoproterenol or any pure -agonist a poor inotropic choice in most situations. Its main cardiovascular impact is an increase in cardiac output because of elevated myocardial contractility. A decline in peripheral vascular resistance caused by 2 activation usually prevents much of an increase in arterial blood pressure. Left ventricular filling strain decreases, whereas coronary blood flow increases. Fenoldopam has been proven to exert hypotensive results characterized by a decrease in peripheral vascular resistance, together with a rise in renal blood circulate, diuresis, and natriuresis. It is indicated for sufferers present process cardiac surgery and aortic aneurysm restore with potential danger of perioperative kidney impairment. Fenoldopam exerts an antihypertensive impact, however helps to preserve renal blood circulate.
British Indian Lemongrass (Lemongrass). Adalat. - How does Lemongrass work?
- Stomach and intestinal spasms, stomach ache, high blood pressure, convulsions, pain, vomiting, cough, rheumatism, fever, common cold, exhaustion, headache, use as an antiseptic and astringent, and other uses.
- Are there safety concerns?
- What is Lemongrass?
- Dosing considerations for Lemongrass.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96704
Buy cheap adalat 20mg on-lineThe deep lymphatic vessels from the foot comply with the principle blood vessels: fibular blood pressure guidelines 2015 buy discount adalat 20mg line, anterior and posterior tibial hypertension nclex questions generic adalat 20 mg on line, popliteal blood pressure medication young age best 20 mg adalat, and femoral veins blood pressure 5545 20mg adalat overnight delivery. Lymphatic vessels from them comply with the femoral vessels, carrying lymph to the deep inguinal lymph nodes. Surface Anatomy of Ankle and Foot Regions the tendons within the ankle region could be recognized satisfactorily only when their muscles are appearing. The fibularis longus tendon can be palpated so far as the cuboid, and then, it disappears because it turns into the only real. The fibularis brevis tendon can easily be traced to its attachment to the dorsal floor of the tuberosity on the bottom of the fifth metatarsal. With toes actively prolonged, the small fleshy stomach of the extensor digitorum brevis may be seen and palpated anterior to the lateral malleolus. Its position should be observed and palpated so that it is probably not mistaken subsequently for an irregular edema (swelling). The tendon of the extensor hallucis longus, obvious when the nice toe is prolonged in opposition to resistance, could also be followed to its attachment to the base of the distal phalanx of the good toe. The tendons of the extensor digitorum longus may be adopted simply to their attachments to the lateral 4 toes. The tendon of the fibularis tertius may also be traced to its attachment to the base of the 5th metatarsal. It may end result from working and high-impact aerobics, especially when inappropriate footwear is worn. The ache is commonly most extreme after sitting and when starting to walk in the morning. It often dissipates after 5�10 minutes of activity and often recurs following relaxation. Point tenderness is located on the proximal attachment of the aponeurosis to the medial tubercle of the calcaneus and on the medial surface of this bone. The ache will increase with passive extension of the good toe and may be further exacerbated by dorsiflexion of the ankle and/or weight bearing. Usually, a bursa develops on the end of the spur that may also turn out to be inflamed and tender. A neglected puncture wound might lead to an in depth deep infection, leading to swelling, ache, and fever. A well-established infection in one of the enclosed fascial or muscular areas normally requires surgical incision and drainage. When attainable, the incision is made on the medial side of the foot, passing superior to the abductor hallucis to allow visualization of crucial neurovascular constructions, whereas avoiding production of a painful scar in a weight-bearing area. Contusion and tearing of muscle fibers and associated blood vessels end in a hematoma (clotted extravasated blood), producing edema anteromedial to the lateral malleolus. Sural Nerve Grafts Pieces of the sural nerve are often used for nerve grafts in procedures corresponding to repairing nerve defects ensuing from wounds. Because of the variations within the stage of formation of the sural nerve, the surgeon might should make incisions in both legs after which select the better specimen. In thin people, these branches can usually be seen or felt as ridges beneath the skin when the foot is plantarflexed. Injections of an anesthetic agent around these branches in the ankle area, anterior to the palpable portion of the fibula, anesthetize the skin on the dorsum of the foot (except the online between and adjacent surfaces of the first and 2nd toes) more broadly and effectively than more native injections on the dorsum of the foot for superficial surgical procedure. The lateral side of the only of the foot is stroked with a blunt object, corresponding to a tongue depressor, starting on the heel and crossing to the base of the great toe. Slight fanning of the lateral four toes and dorsiflexion of the great toe is an irregular response (Babinski sign), indicating brain damage or cerebral disease, besides in infants. Medial Plantar Nerve Entrapment Compressive irritation of the medial plantar nerve because it passes deep to the flexor retinaculum, or curves deep to the abductor hallucis, could cause aching, burning, 1778 numbness, and tingling (paresthesia) on the medial side of the sole of the foot and in the region of the navicular tuberosity. Medial plantar nerve compression might occur during repetitive eversion of the foot. A diminished or absent dorsalis pedis pulse often suggests vascular insufficiency resulting from arterial illness. The 5 P signs of acute arterial occlusion are ache, pallor, paresthesia, paralysis, and pulselessness. Some healthy adults (and even children) have congenitally nonpalpable dorsalis pedis pulses; the variation is often bilateral. In these cases, the dorsalis pedis artery is replaced by an extended perforating fibular artery of smaller caliber than the everyday dorsalis pedis artery, however operating in the same location. Ligation of the deep arch is difficult because of its depth and the constructions that encompass it. Lymphadenopathy Infections of the foot might unfold proximally, inflicting enlargement of the popliteal and inguinal lymph nodes (lymphadenopathy). Infections on the lateral facet of the foot initially produce enlargement of popliteal lymph nodes (popliteal lymphadenopathy); later, the inguinal lymph nodes could enlarge. Inguinal lymphadenopathy without popliteal lymphadenopathy may result from an infection of the medial facet of the foot, leg, or thigh; nonetheless, enlargement of those nodes can also result from an infection or tumor in the vulva, penis, scrotum, perineum, and gluteal area and from terminal elements of the urethra, anal canal, and vagina. Nerves of foot: the plantar intrinsic muscle tissue are innervated by the medial and lateral plantar nerves, whereas the dorsal muscle tissue are innervated by the deep fibular nerve. The latter receives innervation from the deep fibular nerve after it supplies the muscle tissue on the dorsum of the foot. Arteries of foot: the dorsal and plantar arteries of the foot are terminal branches of the anterior and posterior tibial arteries, respectively. It additionally contributes to formation of the deep plantar arch through its terminal deep plantar artery. Efferent vessels of foot: Venous drainage of the foot primarily follows a superficial route, draining to the dorsum of the foot after which medially via the great saphenous vein or laterally by way of the small saphenous veins. The decrease limb joints are (A) these of the pelvic girdle connecting the free lower limb to the vertebral column, (B) the knee and tibiofibular joint, and (C) tibiofibular syndesmosis, ankle joint, and the various joints of the foot. During standing, the entire weight of the upper body is transmitted by way of the hip bones to the heads and necks of the femora. The joint was disarticulated by slicing the ligament of the head of the femur and retracting the top from the acetabulum. The transverse acetabular ligament is retracted superiorly to present the obturator canal, which transmits the obturator nerve and vessels passing from the pelvic cavity to the medial thigh. Except for the despair or fovea for the ligament of the femoral head, all the femoral head is roofed with articular cartilage, which is thickest over weight-bearing areas. The acetabular rim and lunate floor kind approximately three quarters of a circle; the missing inferior segment of the circle is the acetabular notch. This superior view of the hip joint demonstrates the medial and reciprocal pull of the peri-articular muscular tissues (medial and lateral 1784 rotators; reddish brown arrows) and intrinsic ligaments of the hip joint (gray arrows) on the femur. Relative strengths are indicated by arrow width: anteriorly, the muscle tissue are much less ample, but the ligaments are sturdy; posteriorly, the muscular tissues predominate. Parallel fibers linking two discs resemble those making up the tube-like fibrous layer of the hip joint capsule. When one disc (the femur) rotates relative to the opposite (the acetabulum), the fibers turn into increasingly indirect and draw the 2 discs together. Similarly, extension of the hip joint winds (increases the obliquity of) the fibers of the fibrous layer, pulling the pinnacle and neck of the femur tightly into the acetabulum, growing the steadiness of the joint.
Discount adalat 20mg with visaProximally blood pressure chart dot buy generic adalat 30 mg line, the aponeurosis receives fleshy fibers of the soleus directly on its deep surface arteria y arteriola purchase 30 mg adalat free shipping, however distally hypertension medications order 20 mg adalat free shipping, the soleus fibers become tendinous blood pressure 300 150 buy adalat 20mg otc. The tendon thus becomes thicker (deeper) however narrower as it descends till it becomes basically round in cross-section superior to the calcaneus. It then widens as it inserts on the posterior floor of the calcaneal tuberosity. The calcaneal tendon usually spirals 1 / 4 flip (90�) throughout its descent, so that the gastrocnemius fibers attach laterally and the soleal fibers attach medially. Although they share a standard tendon, the 2 muscular tissues of the triceps surae are able to appearing alone, and often do so: "You stroll with the soleus however win the lengthy jump with the gastrocnemius. A subcutaneous calcaneal bursa, situated between the skin and the calcaneal tendon, allows the pores and skin to move over the taut tendon. A deep bursa of the calcaneal tendon (retrocalcaneal bursa), positioned between the tendon and the calcaneus, allows the tendon to glide over the bone. It is a fusiform, two-headed, two-joint 1723 muscle with the medial head slightly bigger and increasing more distally than its lateral companion. The heads come together at the inferior margin of the popliteal fossa, the place they form the inferolateral and inferomedial boundaries of this fossa. Because its fibers are largely of the white, fast-twitch (type 2) selection, contractions of the gastrocnemius produce speedy actions during working and leaping. It features most successfully when the knee is extended (and is maximally activated when knee extension is combined with dorsiflexion, as in the sprint start). The soleus has a continuous proximal attachment in the shape of an inverted U to the posterior aspects of the fibula and tibia and a tendinous arch between them, the tendinous arch of soleus (L. The popliteal artery and tibial nerve exit the popliteal fossa by passing by way of this arch, the popliteal artery concurrently bifurcating into its terminal branches, the anterior and posterior tibial arteries. The soleus is thus an antigravity muscle (the predominant plantarflexor for standing and strolling), which contracts antagonistically but cooperatively (alternately) with the dorsiflexor muscles of the leg to maintain 1725 balance. This vestigial muscle is absent in 5�10% of individuals and is highly variable in size and type when present (most commonly a tapering slip in regards to the dimension of the small finger). It acts with the gastrocnemius however is insignificant as both a flexor of the knee or a plantarflexor of the ankle. The plantaris has been considered to be an organ of proprioception for the larger plantarflexors, as it has a excessive density of muscle spindles (receptors for proprioception). The popliteus acts on the knee joint, whereas the opposite muscular tissues plantarflex the ankle with two persevering with on to flex the toes. However, because of their smaller size and the shut proximity of their tendons to the axis of the ankle joint, the "nontriceps" plantarflexors collectively produce solely about 7% of the whole force of plantarflexion, and on this, the fibularis longus and brevis are most significant. The foot is raised as within the push off section of walking, demonstrating the place of the plantarflexor tendons as they cross the ankle. Observe the sesamoid bone appearing as a "foot stool" for the first metatarsal, giving it further height and defending the flexor hallucis longus tendon. This view demonstrates the disposition of the deep plantarflexor tendons in the sole of the foot. Proximally, its tendinous attachment to the lateral aspect of the lateral femoral condyle and its broader attachment to the lateral meniscus occur between the fibrous layer and the synovial membrane of the joint capsule of the knee. When standing with the knees locked in the absolutely prolonged place, the popliteus acts to rotate the femur laterally 5� on the tibial plateaus, releasing the knee from its close-packed or locked position in order that flexion can occur. When the foot is off the ground and the knee is flexed, the popliteus can aid the medial hamstrings (the "semi-muscles") in rotating the tibia medially beneath the femoral condyles. When barefoot, this thrust is delivered by the nice toe; however with soled sneakers on, it turns into part of the thrust of plantarflexion delivered by the forefoot. The tendon then crosses deep to the tendon of the flexor digitorum longus within the sole of the foot. These bones defend the tendon from the pressure of the top of the 1st metatarsal bone. While standing (especially on one foot), nevertheless, the two muscle tissue may cooperate to depress the lateral side of the foot and pull medially on the leg as wanted to counteract lateral leaning for stability. Postero-inferior to the medial malleolus, the tibial nerve divides into the medial and lateral plantar nerves. The sural nerve provides the pores and skin of the lateral and posterior a part of the inferior third of the leg and the lateral aspect of the foot. It begins on the distal border of the popliteus, as the popliteal artery passes deep to the tendinous arch of the soleus and simultaneously bifurcates into its terminal branches. Close to its origin, the posterior tibial artery offers rise to its largest department, the fibular artery, which runs lateral and parallel to it, also within the deep subcompartment. During its descent, the posterior tibial artery is accompanied by the tibial nerve and veins. Deep to the flexor retinaculum and the origin of the abductor hallucis, the posterior tibial artery divides into medial and lateral plantar arteries, the arteries of the only of the foot. The fibular artery gives muscular branches to the popliteus and different muscle tissue in both the posterior and the lateral compartments of the leg. Distally, the fibular artery offers rise to a perforating branch and terminal lateral malleolar and calcaneal branches. The perforating department pierces the interosseous membrane and passes to the dorsum of the foot, where it anastomoses with the arcuate artery. The lateral calcaneal branches provide the heel, and the lateral malleolar department joins other malleolar branches to type a peri-articular arterial anastomosis of the ankle. The circumflex fibular artery arises from the origin of the anterior or posterior tibial artery on the knee and passes laterally over the neck of the fibula to the anastomoses across the knee. This oval elevation indicates the extent of the head of the fibula and the bifurcation of the popliteal artery into the anterior and posterior tibial arteries. Extensors and flexors of toes are being contracted concurrently, demonstrating extensor tendons with out elevating toes from floor. The patellar ligament may be felt because it extends from the inferior border of the 1734 apex of the patella. When the knee flexes to a right angle, a depression could also be felt on each side of the patellar ligament. The tendon of the biceps femoris may be traced by palpating its distal attachment to the lateral facet of the top of the fibula. The nerve is indicated by a line alongside the biceps femoris tendon, posterior to the pinnacle of the fibula, and around the lateral side of the fibular neck to its anterior aspect, simply distal to the fibular head. The medial floor of the shaft of the tibia can also be subcutaneous, except at its proximal end. Its inferior third is crossed obliquely by the good saphenous vein as it passes proximally to the medial facet of the knee.
Buy adalat 20 mg on-lineUnlike older fashions pulse pressure buy discount adalat 30mg on line, some newer anesthesia machines measure and report widespread outlet gas flows quercetin and blood pressure medication buy adalat 30mg online. An antidisconnect retaining gadget is used to prevent accidental detachment of the gas outlet hose that connects the machine to the respiration circuit heart attack hill 20 mg adalat sale. The oxygen flush valve offers a high flow (35�75 L/min) of oxygen on to blood pressure medication nifedipine buy discount adalat 30 mg line the common gas outlet, bypassing the flowmeters and vaporizers. For this reason, the flush valve should be used cautiously whenever a patient is linked to the respiration circuit. Moreover, inappropriate use of the flush valve (or a situation of caught valve) could end in backflow of gases into the low-pressure circuit, inflicting dilution of inhaled anesthetic focus. Some machines use a second-stage regulator to drop the oxygen flush stress to a lower stage. The elements and use of the circle system had been beforehand discussed (see Chapter 3). It is important to observe that fuel composition at the widespread gas outlet can be controlled precisely and quickly by changes in flowmeters and vaporizers. Use of excessive fuel circulate charges during induction and emergence decreases the consequences of such variables and might diminish the magnitude of discrepancies between fresh fuel outlet and circle system anesthetic concentrations. Note gas flow throughout A: spontaneous inspiration, B: handbook inspiration ("bagging"), and C: exhalation (spontaneous or bag ventilation). In most machines, the widespread gas outlet is hooked up to the breathing circuit just previous the exhalation valve to stop artificially excessive exhaled tidal quantity measurements. When spirometry measurements are made on the Y-connector, contemporary fuel move can enter the circuit on the patient aspect of the inspiratory valve. The advantages of those designs embrace decreased chance of respiratory circuit misconnects, disconnects, kinks, and leaks. The smaller quantity of compact machines can even assist conserve gas circulate and unstable anesthetics and permit faster modifications in breathing circuit gasoline focus. Spirometers Spirometers, also known as respirometers, are used to measure exhaled tidal volume in the breathing circuit on all anesthesia machines, sometimes close to the exhalation valve. The flow of gasoline across vanes within the respirometer causes their rotation, which is measured electronically, photoelectrically, or mechanically. During positive-pressure air flow, modifications in exhaled tidal volumes usually characterize adjustments in ventilator settings, however can be due to circuit leaks, disconnections, or ventilator malfunction. These spirometers are prone to errors brought on by inertia, friction, and water condensation. For instance, Wright respirometers under-read at low flow charges and over-read at high move charges. Furthermore, the measurement of exhaled tidal volumes at this location within the expiratory limb consists of gas that had been misplaced to the circuit (and not delivered to the patient; mentioned below). The distinction between the volume of fuel delivered to the circuit and the amount of gasoline truly reaching the affected person turns into very significant with long, compliant respiratory tubes; fast respiratory charges; and elevated airway pressures. Oxygen Analyzers General anesthesia should not be administered without an oxygen analyzer in the respiration circuit. Three types of oxygen analyzers can be found: polarographic (Clark electrode), galvanic (fuel cell), and paramagnetic. The first two methods make the most of electrochemical sensors that include cathode and anode electrodes embedded in an electrolyte gel separated from the sample fuel by an oxygenpermeable membrane (usually Teflon). The galvanic and polarographic sensors differ in the composition of their electrodes and electrolyte gels. In addition, their response time is quick sufficient to differentiate between impressed and expired oxygen concentrations. A hot-wire anemometer makes use of a nice platinum wire, electrically heated at a continuing temperature, contained in the gasoline flow. The cooling effect of increasing fuel flow on the wire electrode causes a change in electrical resistance. In a constant-resistance anemometer, gas circulate is decided from the present wanted to keep a relentless wire temperature (and resistance). Disadvantages embody an lack of ability to detect reverse circulate, much less accuracy at larger circulate rates, and the possibility that the heated wire could also be a potential ignition supply for fireplace within the respiratory manifold. Ultrasonic circulate sensors rely on discontinuities in gas circulate generated by turbulent eddies in the circulate stream. Upstream and downstream ultrasonic beams, generated from piezoelectric crystals, are transmitted at an angle to the fuel stream. The Doppler frequency shift within the beams is proportional to the move velocities in the respiration circuit. One measures flow at the inspiratory port of the respiration system, and the opposite measures flow at the expiratory port. The changes in fuel flows in the course of the inspiratory and expiratory phases help the ventilator to modify and supply a relentless tidal volume. However, due to extreme condensation, sensors can fail when used with heated humidified circuits. A pneumotachograph is a fixed-orifice flowmeter that may perform as a spirometer. A parallel bundle of small-diameter tubes in chamber (Fleisch pneumotachograph) or mesh display screen provides a slight resistance to airflow. The stress drop throughout this resistance is sensed by a differential pressure transducer and is proportional to the circulate fee. Moreover, analysis of pressure, volume, and time relationships can yield doubtlessly useful details about airway and lung mechanics. Modifications have been required to overcome inaccuracies as a result of water condensation and temperature modifications. Gas flowing through the Pitot tube (flow sensor tube) creates a pressure difference between the move sensor lines. This pressure differential is used to measure move, move direction, and airway strain. Respiratory gases are repeatedly sampled to correct the circulate reading for changes in density and viscosity. Circuit Pressure A strain gauge or digital sensor is always used to measure breathing-circuit stress someplace between the expiratory and inspiratory unidirectional valves; the precise location is determined by the mannequin of anesthesia machine. The most accurate measurements of both inspiratory and expiratory pressures could be obtained from the 6 Y-connection. Despite this buildup in airway stress, a strain gauge on the absorber will read zero because of the intervening one-way valve. Some machines have incorporated auditory suggestions for pressure adjustments during ventilator use. At the same time, if it is closed an excessive amount of or is totally closed, a progressive rise in strain may result in pulmonary barotrauma (eg, pneumothorax) or hemodynamic compromise, or each. Relative humidity is the ratio of the actual mass of water current in a volume of gas to the utmost amount of water potential at a particular temperature.
Generic 30mg adalat amexEvidence means that no less than some groups of high-risk patients could do better with blood cardioplegia blood pressure medication for adhd 20mg adalat mastercard. Certainly arteria carotis interna cheap adalat 30 mg with amex, oxygenated blood cardioplegia could comprise extra oxygen than crystalloid cardioplegia hypertension yoga exercises purchase adalat 30mg amex. Because cardioplegia may not attain areas distal to high-grade coronary obstructions (the areas that want it most) venice arrhythmia 2013 generic adalat 30 mg otc, many surgeons administer retrograde cardioplegia via a coronary sinus catheter. Some centers have reported that the mix of antegrade plus retrograde cardioplegia is superior to either approach alone. Cardiac surgery carried out with true normothermia (rather than tepid bypass) raises additional considerations about loss of the potentially protecting effects of systemic hypothermia against cerebral harm. As mentioned previously, with prolonged myocardial ischemic times (cross-clamp time), reperfusion of the myocardium can result in extensive cell damage, speedy accumulation of intracellular calcium, and probably irreversible cellular necrosis. This process has long been attributed to accumulation of oxygen-derived free radicals. Free radical scavengers, corresponding to mannitol, could assist decrease reperfusion damage and are typical constituents of cardioplegic options and bypass "priming" options. Just previous to reperfusion, the heart could additionally be perfused by a reduced potassium cardioplegic resolution that serves to wash out amassed metabolic byproducts. Alternatively, a "hot shot" or warm blood cardioplegic resolution could additionally be administered to wash out byproducts and replenish metabolic substrates. Reperfusion pressures should be managed closely due to altered coronary autoregulation. Inadequate myocardial safety or inadequate washout and restoration from cardioplegia can lead to asystole, atrioventricular conduction block, or a poorly contracting coronary heart on the finish of bypass. Excessive volumes of hyperkalemic cardioplegic options may produce persisting systemic hyperkalemia. Although calcium salt administration partially offsets hyperkalemia, excessive calcium can promote and improve myocardial injury. In the standard patient, myocardial performance improves with time as the contents of the cardioplegia are cleared from the guts. Elevated concentrations of catecholamines, cortisol, arginine vasopressin, and angiotensin are noticed. Multiple humoral methods are also activated, together with complement, coagulation, fibrinolysis, and the kallikrein system. A systemic inflammatory response much like that seen with sepsis and trauma can develop. When this response is intense or extended, sufferers can develop the identical complications as are seen with sepsis or trauma, together with generalized edema, acute respiratory distress syndrome, coagulopathy, and acute kidney failure. The resulting platelet dysfunction likely increases perioperative bleeding and potentiates other coagulation abnormalities (activation of plasminogen and the inflammatory response beforehand described). Leukocyte-depleted blood cardioplegia has been shown to improve myocardial preservation in some studies. Administration of free radical scavengers such as high-dose nutritional vitamins C and E and mannitol has improved consequence in some studies, but stays investigational. Unfortunately, it elevated mortality and is no longer available in North America. Heparin doubtlessly alters protein binding of medicine and ions by releasing and activating lipoprotein lipase, which hydrolyzes plasma triglycerides into free fatty acids; the latter can competitively inhibit drug binding to plasma proteins and bind free calcium ions. The similar rules apply whether these patients are present process cardiac or noncardiac surgery. An necessary distinction is that sufferers undergoing cardiac procedures will by defi4 nition have advanced disease. Fortunately, not like noncardiac surgical procedure, cardiac surgery improves cardiac function in the majority of sufferers, and these patients have often been extensively evaluated before being provided surgical repair. The anesthetic preoperative analysis must also embody a give attention to pulmonary, neurological, and kidney perform, as preoperative impairment of those organ systems predisposes sufferers to myriad postoperative issues. Preinduction Period Premedication the prospect of coronary heart surgical procedure is frightening, and comparatively "heavy" premedication was usually given in the past (see Chapter 21). Benzodiazepine sedativehypnotics (diazepam, 5�10 mg orally), alone or together with an opioid (morphine, 5�10 mg intramuscularly or hydromorphone, 1�2 mg intramuscularly), had been usually used. However, in current follow most patients obtain no sedative-hypnotic premedication until their arrival on the surgical unit, at which time many will obtain small doses of intravenous midazolam. Longer acting premedicant brokers (eg, lorazepam) are avoided by most practitioners to allow fast-tracking of patients via their restoration. Drug infusions should ideally be given into a central catheter, ideally immediately into the catheter or into the injection port closest to the catheter (to reduce dead space). Multilumen central venous catheters and multilumen pulmonary artery catheter introducer sheaths permit for a number of drug infusions with simultaneous measurement of vascular pressures. One intravenous port must be solely for drug infusions; drug and fluid boluses should be administered via another site. Preparation the most effective practitioners of cardiac anesthesia formulate a easy anesthetic plan that includes enough preparations for contingencies. Preparation, group, and attention to element permit one to deal more effectively with unexpected intraoperative issues. The anesthesia machine, monitors, infusion pumps, and blood warmer ought to all be checked before the patient arrives. Drugs-including anesthetic and vasoactive agents-should be immediately available. Many clinicians prepare one vasoconstrictor and one vasodilator infusion before the beginning of the procedure. Arterial Blood Pressure In addition to all primary monitoring, arterial cannulation is always performed either prior to or immediately after induction of anesthesia. Radial arterial catheters may often give falsely low readings following sternal retraction on account of compression of the subclavian artery between the clavicle and the primary rib. The radial artery on the side of a previous brachial artery cutdown ought to be prevented, because its use is associated with a larger incidence of arterial thrombosis and wave distortion. Other useful catheterization websites embody the brachial, femoral, and axillary arteries. Venous Access Cardiac surgical procedure is sometimes associated with giant and rapid blood loss, and with the need for a number of drug infusions. Ideally, two large-bore (16-gauge or larger) intravenous catheters should be positioned. One of these must be in a large central vein, normally an internal or exterior jugular or subclavian vein. Central venous cannulations could additionally be completed whereas the affected person is awake however sedated or after induction of anesthesia.
Discount adalat 20 mg with amexThey are normally thinner in females than in males and are thinner in youngsters and elderly individuals hypertension of the eye order adalat 30mg mastercard. The diplo� is cancellous bone containing red bone marrow during life blood pressure chart in pdf generic 30mg adalat visa, through which run canals shaped by diploic veins arrhythmia update 2014 discount adalat 20 mg mastercard. Relatively skinny (but mostly curved) flat bones present the required power to keep cavities and protect their contents blood pressure of 150/90 discount 20 mg adalat overnight delivery. However, in addition to housing the brain, the bones of the neurocranium (and processes from them) present proximal attachment for the sturdy muscles of mastication that attach distally to the mandible. Consequently, excessive traction forces happen across the nasal cavity and orbits that are sandwiched between. The primary buttresses are the frontonasal buttress, extending from the area of the canine teeth between the nasal and the orbital cavities to the central frontal bone, and the zygomatic arch�lateral orbital margin buttress from the region of the molars to the lateral frontal and temporal bones. Similarly, occipital buttresses transmit forces received lateral to the foramen magnum from the vertebral column. Perhaps to compensate for the denser bone required for these buttresses, some areas of the skull not as mechanically careworn become pneumatized (air filled). The buttresses are thicker portions of cranial bone that transmit forces around weaker areas of the cranium. The giant variety of regions into which the relatively small space of the face is divided (eight) displays its useful complexity and private importance, as do annual expenditures for elective aesthetic surgical procedure. Except for the auricular area, which incorporates the external ear, the names of the regions of the neurocranial portion of the pinnacle correspond to the underlying bones or bony features: frontal, parietal, occipital, temporal, and mastoid regions. The viscerocranial portion of the pinnacle contains the facial region, which is divided into five bilateral and three median areas related to superficial options (oral and buccal regions), to deeper gentle tissue formations (parotid region), and to skeletal features (orbital, infra-orbital, nasal, zygomatic, and psychological regions). The remainder of this chapter discusses several of those regions intimately, in addition to some deep regions not represented on the surface. The surface anatomy of these areas will be discussed with the description of every region. The problems of head injuries embrace hemorrhage, an infection, and injury to the mind. Disturbance in the degree of consciousness is the most common symptom of head damage. Almost 10% of all deaths within the United States are brought on by injury, and roughly half of traumatic deaths contain the brain (Louis et al. The major explanation for brain damage varies; nonetheless, motorized vehicle and motorbike accidents are outstanding. Headaches and Facial Pain Few complaints are extra common than complications and facial ache. Although often benign and regularly related to rigidity, fatigue, or delicate fever, headaches might indicate a severe intracranial drawback similar to a mind tumor, subarachnoid hemorrhage, or meningitis. Localized aches have particular names, corresponding to earache (otalgia) and toothache (odontalgia). A sound data of the medical anatomy of the top helps in understanding the causes of complications and facial ache. This redness of the skin overlaying the zygomatic process (malar eminence) is related to a rise in temperature in various fevers occurring with certain illnesses, such as tuberculosis and systemic lupus erythematosus disease. Le Fort I fracture: extensive variety of horizontal fractures of the maxillae, passing superior to the maxillary alveolar process. As a end result, the 1903 entire central part of the face, together with the onerous palate and alveolar processes, is separated from the relaxation of the cranium. Concurrent fracturing of the zygomatic arches causes the maxillae and zygomatic bones to separate from the relaxation of the cranium. Fractures of Mandible A broken mandible normally involves two fractures, which incessantly occur on reverse sides of the mandible. Line A, fracture of the coronoid course of; line B, fracture of the neck of the mandible; line C, fracture of the angle of the mandible; line D, fracture of the physique of the mandible. Following complete loss or extraction of maxillary enamel, the tooth sockets start to fill in with bone, and the alveolar course of begins to resorb. Similarly, extraction of mandibular enamel causes the bone of the alveolar half to resorb. In some circumstances, the psychological foramina disappear, exposing the mental nerves to harm. Loss of all the tooth leads to a lower in the vertical facial dimension and mandibular prognathism (overclosure). Deep creases in the facial skin additionally appear that cross posteriorly from the corners of the mouth. Fractures of Calvaria the convexity of the calvaria distributes and thereby normally minimizes the consequences of a blow to the top. Linear calvarial fractures, essentially the most frequent sort, usually happen at the level of influence, however fracture traces often radiate away from it in two or extra instructions. If the world of the calvaria is thick at the website of impact, the bone might bend inward without fracturing. However, a fracture may occur far from the site of direct trauma the place the calvaria is thinner. In a contrecoup (counterblow) fracture, no fracture occurs on the level of impression, but one occurs on the other aspect of the skull. Because the adult pericranium (periosteum of cranium) has poor osteogenic (bone-forming) properties, little regeneration occurs after bone loss. Surgically produced bone flaps are put again into place and wired to different parts of the calvaria or held in place temporarily with metallic plates. Reintegration is most profitable when the bone is reflected with its overlying muscle and pores and skin, so that it retains its own blood provide through the process and after repositioning. Development of Cranium the bones of the calvaria and a few components of the cranial base develop by intramembranous ossification. At delivery, the bones of the calvaria are clean and unilaminar; no diplo� is current. The cranium of a neonate is disproportionately giant in comparison with different components of the skeleton; nevertheless, the facial facet is small compared to the calvaria, which types roughly one eighth of the cranium. The massive measurement of the calvaria in infants results from precocious growth and improvement of the brain and eyes. The smallness of the face results from the rudimentary growth of the maxillae, mandible, and paranasal sinuses (air-filled bone cavities), the absence of erupted enamel, and the small measurement of the nasal cavities. The halves of the frontal bone in the neonate are separated by the frontal suture, the frontal and parietal bones are separated by the coronal suture, and the maxillae and mandibles are separated by the intermaxillary suture and mandibular symphysis (secondary cartilaginous joint), respectively. Thus, the facial nerves could additionally be injured by forceps during a difficult supply or later by an incision posterior to the auricle of the exterior ear. The mastoid processes kind progressively through the 1st year because the sternocleidomastoid muscular tissues complete their development and pull on the petromastoid components of the temporal bones. The bones of the calvaria of neonates are separated by fontanelles (fibrous membranes; palpable deep to the scalp, these are perceived as "soft spots"). They embrace the anterior and posterior fontanelles and the paired sphenoidal and mastoid fontanelles.
References - Choo KE, Tan KK, Chuah SP, et al. Hemorrhagic disease of newborn and infants: a study of hospitalized children in Kelanatan, Malaysia. Ann Trop Pediatr. 1994;14:231-7.
- Spiegel K, Tasali E, Penev P, et al: Brief communication: sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels and increased hunger and appetite, Ann Intern Med 141:846n850, 2004.
- Darney KJ Jr, Zirkin BR, Ewing LL: Testosterone autoregulation of its biosynthesis in the rat testis: inhibition of 17 alpha-hydroxylase activity, J Androl 17:137n142, 1996.
- Van Cangh, P.J., Nesa, S., De Groote, P. Current indications for endopyelotomy. Braz J Urol 2000;26:54-63.
|