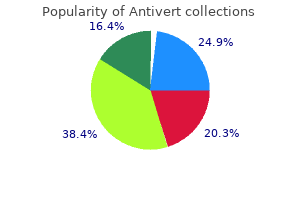
Antivert
Phillip Fairweather, M.D. - Clinical Assistant Professor
- Mount Sinai School of Medicine
- New York, NY
- Department of Emergency Medicine
- Elmhurst Hospital Center
- Elmhurst, NY
Antivert: 25 mg
Purchase antivert 25 mg onlineThe arc-radius body design has the benefit of being extra versatile in the operating room and permitting for higher intraoperative adjustment of the lead entry level 92507 treatment code buy antivert 25 mg low price. However symptoms 5 weeks into pregnancy buy antivert 25 mg low cost, frameless systems are much less versatile intraoperatively medicine nobel prize 2015 antivert 25mg, affording a narrower range of lead entry factors and restricted capacity to regulate lead trajectories if preliminary planning was suboptimal symptoms 9 days post ovulation antivert 25mg without prescription. To date there has been no head-to-head comparability of the safety and efficacy of those completely different approaches to stereotactic lead placement. Surgical Procedure the pores and skin incision and burr holes are made underneath local anesthesia or gentle sedation, and the bone sealed with bone wax to cut back the risk of venous air embolism through uncovered skull veins. A durotomy and pial incision are carried out to accommodate the electrode guide tubes, and hemostasis is assured. In planning the trajectory, the objective is to place the lead exactly at the target location while avoiding eloquent tissue and vasculature. At most facilities, the goal is further refined through microelectrode recording, although physiology protocols range substantially among surgeons. A smaller recording microelectrode is advanced via the cannula to the goal, recording alongside the way to confirm attribute physiological transitions between grey and white matter along the trajectory and attribute neural responses to movement and sensory stimulation. Multiple electrode passes could additionally be used sequentially or simultaneously till the optimal goal is recognized. Microstimulation can be utilized via the mapping electrode (or a separate stimulating sheath) to assess for clinical results of stimulation. Once the goal has been recognized, the persistent stimulating electrode is placed by way of the identical cannula, which minimizes brain shift between the physiology mapping and electrode placement. After placement of the leads, macrostimulation is applied to every of the lead contacts in flip to assess for the voltages at which clinical advantages and side effects are seen. If the stimulation leads to inadequate scientific profit or intolerable unwanted facet effects at low voltages, the surgeon can move the lead and retest. We observed a reduced rate of hemorrhage after implementing this design12; nonetheless, this configuration not allows microstimulation via the outer protecting sheath. Affixing the lead solely with bone cement (methyl methacrylate) is insufficient and may end up in subsequent lead migration. Our practice is to safe the lead with bone cement, a silk ligature fastened to a small gap drilled in the medial fringe of the burr gap, and a titanium miniplate. When utilizing a titanium plate, care is taken to not overtighten the plate, which may find yourself in fracture of the lead. During this era lead place may also migrate barely as postoperative pneumocephalus resolves. For these reasons, therapeutic electrical stimulation is typically initiated 2 to 4 weeks after lead implantation. Although this increases affected person discomfort, it considerably aids implantation concentrating on as the results of intraoperative macrostimulation are more evident when off medicine. If a patient is unable to take oral treatment secondary to dysphagia, for example, enteral entry via nasogastric tube can be used to administer most medicines. Lastly, intravenous formulations of the dopamine agonist, apomorphine, can be found however must be utilized in session with a neurologist who has experience with these medicines, their unwanted side effects, and titration. There are case stories of neuroleptic malignant syndrome (also known as parkinsonism-hyperpyrexia syndrome in this context) after overnight withdrawal of dopaminergic remedy. Although uncommon, the surgical team ought to pay consideration to the likelihood because the outcome is determined by prompt treatment with supportive take care of fever and autonomic instability, resumption of dopaminergic therapy (� addition of bromocriptine), and the addition of the skeletal muscle relaxant dantrolene. Differences in the reported fee of hemorrhage between research are in part associated to the frequency, modality, and high quality of postoperative imaging with the ability to detect smaller asymptomatic hemorrhages. In centers that carry out routine postoperative imaging, asymptomatic hemorrhage has been reported after 3. Rates of hemorrhage resulting in long-term neurological deficits lasting longer than 30 days are 0. For intraparenchymal hemorrhage, complication rates per lead implanted are shown in parentheses. The transition level between the electrode and the guide-tube sheath, normally situated 2 to three cm above the target, may be a particularly frequent site of hemorrhage. Identification and management of deep brain stimulation intra- and postoperative urgencies and emergencies. Our practice is to stop recording once the microelectrodes have clearly exited the pallidum to keep away from injury to the optic tracts and vessel-rich choroid fissure. However, hemorrhage causing symptomatic mass impact or hydrocephalus might warrant therapeutic craniotomy or placement of an extraventricular drain. Management consists of identifying and treating reversible hemodynamic, metabolic, and infectious etiologies; judicious use of opiates, benzodiazepines, anticholinergics, and other deliriogenic medications; and nonpharmacologic interventions including encouraging normal sleep�wake cycles and minimizing overnight awakenings. Management is usually supportive with consideration to a workup to identify and handle different etiologies of stroke, together with hypoperfusion, intracranial or carotid stenosis, or cardioemboli. These symptoms may end result from direct tissue damage from lead insertion and postoperative edema. A range of signs have been documented, including aphasia, mutism, visible area deficits, oculomotor palsies, facial palsies, dysphagia, dysarthria, eyelid opening apraxia, paresis, ballism, imbalance, and sensory loss. Psychiatric symptoms together with melancholy, mania, psychosis, impulse control disorders, nervousness, and suicidality also can emerge or worsen,37 a few of which can be stimulation dependent. Seizures may happen secondary to tissue disruption and edema from lead insertion and cortical irritant effects of pneumocephalus or intracranial hemorrhage. In one collection, the presence of hemorrhage, edema, or ischemia on postoperative imaging was associated with a 50-fold elevated risk of seizure; these findings had been more frequent in patients older than 60 years of age and people for whom the lead trajectory was transventricular. A short course of anticonvulsant remedy is cheap, however long-term anticonvulsant remedy is mostly not warranted. Venous Air Embolus If monitored by continuous transthoracic or transesophageal echocardiography, transvenous air embolism has been documented to occur during 7% to 76% of neurosurgical procedures carried out in the sitting position. One potential study utilizing precordial ultrasound monitoring recognized air embolism in 1 of 21 patients (5%). If an air embolism is suspected, one should instantly lower the head of the mattress to at or beneath the extent of the proper atrium and flood the surgical subject with saline. After explantation, topics must be treated with intravenous antibiotics and monitored for indicators of persistent an infection for at least 2 months earlier than hardware is reimplanted. Perioperative respiratory problems, including airway obstruction, aspiration, and nosocomial pneumonia, are reported to happen in 1. It is crucial that the surgical and anesthesia groups are familiar with the stereotactic body and have the necessary tools readily available to manipulate it in case of an airway emergency. Antibiotic choice must be guided by the native surgical-site infection pathogens and sensitivities. Infections that instantly involve hardware are difficult to deal with medically and normally require hardware explantation. In common, the lead extension connector is usually positioned retroauricularly under the scalp and should generally not be placed in the neck as a end result of the larger stresses that result from neck movement.
Order antivert 25mg fast deliveryDirect nerve restore is just potential after clean treatment water on the knee buy 25mg antivert fast delivery, sharp penetrating accidents and should be performed acutely to enable for optimal probability of recovery of function medicine bottle generic antivert 25mg amex. In some instances medicine encyclopedia order antivert 25mg on line, jagged lacerations of the nerve could be tagged for delayed restore medicine kit for babies generic 25mg antivert overnight delivery, which permits for appropriate trimming of the injured nerve stumps and grafting, if necessary. Nerve grafting was launched by Seddon in 196328 and remains essentially the most generally employed technique in brachial plexus reconstruction surgery. The medial cutaneous nerves of the arm and forearm, the radial sensory nerve, and the saphenous nerve from the thigh are generally additionally used. Outcomes after nerve grafting are extremely dependent on the length of the graft, the timing of intervention, presence of scar tissue at the wound website, variety of grafts used, and the presence of a healthy proximal stump obtainable for grafting. Common examples of interpositional nerve grafting include coaptation of C5 spinal nerve to suprascapular nerve or axillary nerve (for shoulder abduction), C6 to musculocutaneous nerve (for elbow flexion), and C7 to triceps or radial nerve (for elbow extension and wrist extension). The supraclavicular incision is on the best and infraclavicular incision on the left of the determine. The ipsilateral neck, thorax, higher extremity, and bilateral decrease extremities (for attainable sural nerve graft in cases of trauma) should be prepped and draped with the upper extremity resting on an arm board desk. The supraclavicular fats pad is mobilized alongside its medial and inferior borders and is retracted laterally. The transverse cervical artery and vein are identified at this degree and are both retracted or ligated and transected. The posterior stomach of the omohyoid muscle is then encountered and likewise retracted. In circumstances of extreme trauma, the nerve will not be visible initially and should require electrical stimulation to induce hemidiaphragm contraction. Care should be taken to protect this fragile neural structure and gently retract it to avoid damage. The phrenic nerve serves as an necessary landmark for identifying the C5 spinal nerve. The C5 spinal nerve may be identified becoming a member of the C6 spinal nerve to form the higher trunk. Exposure of the middle and lower trunks requires C7, C8, and T1 spinal nerve visualization. Similarly, the middle scalene muscle may also include fibrous elements close to the attachment to the first rib. Depending on the extent of injury, extensive neurolysis (360-degree dissection) is then performed on all plexus components. In instances of trauma, the trunks are dissected distally and beneath the clavicle to determine the anterior and posterior divisions and the suprascapular nerve. Infraclavicular brachial plexus exposure via the deltopectoral groove is often necessary in these instances. The surgeon should also recheck for leakage of lymphatic fluid as a outcome of chylothorax could additionally be a major complication. The platysma and subcutaneous layers are closed with interrupted 3-0 Vicryl suture adopted by 4-0 operating subcuticular absorbable suture for the skin. In instances of nerve restore, we keep the arm in a sling for three weeks after which prescribe progressive range-of-motion workouts under supervision of an experienced bodily therapist. In addition, inspiration and expiration views enable for assessment of diaphragmatic paralysis. Clinical Pearls Appropriate affected person choice and correct localization of the lesion utilizing detailed historical past and physical examination stay essentially the most important features of profitable peripheral nerve surgery. Complete dissection of all injured brachial plexus elements, along with intraoperative electrophysiological studies, are essential to establish the optimum surgical management with neurolysis, nerve grafts, and/or nerve transfers. The phrenic nerve is particularly susceptible to retraction harm during exposure of the supraclavicular brachial plexus. Traumatic brachial plexus injuries and administration Perioperative Considerations Key Concepts Imaging research and electrophysiological studies are used in conjunction with the medical examination of the patient to decide the best remedy course. Planning brachial plexus reconstruction surgery requires thorough preoperative and perioperative evaluation. Often, imaging studies along with electrophysiological research are used to supplement the scientific examination of the patient. Among the imaging research, computed tomography myelogram is ready to detect nerve root avulsions with a sensitivity of 85% and a specificity of 95%. Because these findings suggest spontaneous recovery, repeat electrodiagnostic studies are really helpful prior to surgical intervention. Preganglionic injuries can be recognized electrophysiologically as a result of an damage proximal to the dorsal root ganglion will spare distal sensory axons. Intraoperative electrodiagnostic studies are invaluable in brachial plexus reconstruction surgical procedures. Electrical stimulation of the brachial plexus elements could be carried out during surgical procedure to provide the surgeon insight into the relative well being or degeneration of specific nerve fibers. One of essentially the most crucial aspects of brachial plexus reconstruction requires perioperative choice making concerning the goals and timing of surgery. Given that in lots of of these instances few functioning neural elements exist, prioritization of functional restoration turns into paramount. Many authors 44 Management of Traumatic Brachial Plexus Injuries 463 advocate for elbow flexion and shoulder stability as basic priorities for improved end result. With respect to timing of surgical procedure, there has recently been vital curiosity in performing very early nerve transfers and/or nerve grafting, both in the grownup and pediatric populations. This aggressive approach is supported by the natural historical past of neuronal cell death due to axotomy. It is even more essential in preganglionic accidents, in which as much as 80% of motoneurons bear cell demise in animal fashions. These sufferers require early session with a peripheral nerve surgeon to have the ability to decide indications for early brachial plexus exploration or nerve transfer. One of the most common causes for delayed brachial plexus repair is the presence of different associated main injuries, which may distract from the analysis of important nerve harm. This is extra common in high-risk populations, together with diabetic and renal failure sufferers. Seromas and hematomas within the operative areas could be minimized by judicious use of drains. An immediate postoperative chest x-ray is important to assess for pneumothorax and for proof of hemidiaphragm elevation, which indicates ipsilateral phrenic nerve damage. Donor website morbidity from nerve harvesting can be a recognized complication of brachial plexus reconstruction surgery. For instance, intercostal nerve transfers are associated with pleural tear during nerve elevations, occurring in roughly 9% of instances. Additional surgical issues embrace chylothorax, causalgia, and further injury to the plexus, including complete paralysis and full sensory loss.

Order antivert 25 mg with visaRecent advances have considerably improved the understanding of the pathobiology of adrenal proliferation and aldosterone extra in major aldosteronism treatment venous stasis order antivert 25 mg overnight delivery. These mutant channels expressed within the adrenal glomerulosa lose their specificity for potassium and allow inward circulate medicine versed order antivert 25mg otc. The same mutation has been identified as a germline mutation in patients with a uncommon type of adrenal hyperplasia (familial aldosteronism type 3) and ends in massive adrenal hyperplasia spa hair treatment order antivert 25mg free shipping, aldosterone manufacturing symptoms copd trusted 25mg antivert, and extreme hypertension with cardiovascular complications. Levels between 5 and 10 ng/dL are thought-about indeterminate and require both repeat testing or another confirmatory test. The two most common subtypes are bilateral hyperplasia (~60% of cases) and adrenal adenomas (~40% of cases). Rare causes embrace adrenal carcinoma, unilateral adrenal hyperplasia, and glucocorticoid-remediable aldosteronism. Visualization of a small (<3 cm), hypodense (<10 Hounsfield units) adrenal nodule is nearly diagnostic of an adenoma. This is justified by the very low rate of incidental adrenal plenty in this age vary. The take a look at starts with the administration of cosyntropin, which is used to produce maximal cortisol secretion from both adrenal glands to present a great means for "adjustment" of the aldosterone results. I use a continuous infusion of 50 �g/h intravenously beginning 30 minutes earlier than the catheterization and persevering with until the end of the process. Blood is sampled from each of the adrenal glands and a peripheral website (can be the inferior vena cava or an higher extremity vein) and is distributed for each aldosterone and cortisol. Confirmatory checks are designed to doc persistent autonomous production of aldosterone despite using a physiologic factor that strongly suppresses aldosterone secretion. Potassium should be successfully changed in the course of the collection to avoid hypokalemia. We measure urine creatinine (to assess the completeness of the collection), sodium (to verify >200 mEq/day intake), and aldosterone. Urine aldosterone excretion higher than 12 to 14 �g/day is confirmatory, whereas levels lower than 10 �g/day convincingly exclude the diagnosis. A postinfusion aldosterone larger than 10 ng/dL First, every aldosterone and cortisol level must be analyzed as ratios of aldosterone-to-cortisol from each of the three 638 Section12-HypertenSion sampling websites. Second, the aldosterone/cortisol ratio for the best adrenal vein is compared with the left adrenal vein, and both are in contrast with the peripheral ratio. If the aldosterone/cortisol ratio on one of the adrenal veins is bigger than or equal to four times greater than the contralateral aspect, the prognosis of lateralization is made, indicating the presence of an aldosterone-producing adenoma or, rarely, unilateral adrenal hyperplasia. In addition, sufferers with adenomas typically have suppressed secretion from the contralateral aspect (defined as aldosterone/cortisol ratio from the contralateral side decrease than that from the periphery). OtherTesting In the previous, several biochemical tests and nuclear drugs imaging (iodocholesterol) had been used to help in subtype differentiation. In sufferers suspected of having glucocorticoid-remediable aldosteronism (early hypertension, private or family historical past of hemorrhagic strokes or mind aneurysms), the diagnosis ought to be made via formal genetic testing to determine the chimeric gene mutation (between the aldosterone synthase and 11-hydroxylase genes). Patients with an aldosterone-producing adenoma or unilateral adrenal hyperplasia should be provided laparoscopic unilateral adrenalectomy. A current medical trial confirmed that spironolactone was barely better than eplerenone, although the doses might not have been precisely exchangeable. For these patients who develop insupportable unwanted effects to spironolactone, particularly these associated to its antiandrogenic results, I substitute eplerenone utilizing a 2: 1 dosing ratio and twice-daily dosing. The danger of hyperkalemia clearly exists however may be mitigated with the use of smaller doses. Aldosterone synthase inhibitors are under growth and have been tested in patients with main aldosteronism. Thiazide diuretics are often helpful, though potassium levels have to be monitored intently as they may drop precipitously with the thiazide. Paraganglioma is a tumor derived from extraadrenal chromaffin cells of the sympathetic paravertebral and neck ganglia. Pheochromocytomas are almost always biochemically energetic, producing epinephrine, norepinephrine, or dopamine, alone or together. Paragangliomas may be biochemically silent, especially when originating in the neck and base of the cranium. Overall, pheochromocytomas represent approximately 80% to 85% of these tumors, whereas paragangliomas account for roughly 15% to 20%. However, knowledge about their clinical presentation and the suitable strategy to analysis and administration are essential because of the cardiovascular threat they pose by way of severe hypertension. These paroxysms are related to catecholamine release and are clinically characterised by the traditional triad of complications, palpitations, and diaphoresis. Other common signs are nervousness, tremulousness, pallor, pale flushing, and orthostatic hypotension. These developments not solely have diagnostic and genetic counseling relevance but in addition could have treatment implications in the future. The measurement of free metanephrines in serum or urine is the popular diagnostic test. Plasma or urine free metanephrines are acceptable screening measurements, each having an accuracy within the 96% to 99% vary. Sensitivity could be very excessive, though there are shortcomings in specificity due to substances that will trigger falsely elevated ranges. In the case of plasma metanephrines, false-positive normetanephrine could be noticed with acetaminophen (only certain assays), tricyclic antidepressants, methyldopa, phenoxybenzamine, and sulfasalazine, whereas buspirone may elevate plasma metanephrines. The Endocrine Society recommends supine measurements; nonetheless, it recognizes the sensible limitations of this advice, as most laboratories are unable to accommodate this request. The guidelines recommend individual screening for mutations based on the familial distribution, the presence of a defined syndrome, and the guided choice of genes to be examined based on location and biochemical profile of the tumor. Pheochromocytomas can be managed laparoscopically, whereas paragangliomas are normally resected with an open method. All sufferers must be treated medically for at least 1 to 2 weeks in anticipation of surgical procedure. The cornerstone of therapy is an alpha-blocker (either the nonselective phenoxybenzamine or a selective alpha1-blocker, corresponding to doxazosin or terazosin). The analysis and management of metastatic disease are nuanced and past the scope of this chapter. In most circumstances, biochemical screening is repeated 6 months following resection after which yearly. In high-risk patients, corresponding to these with massive pheochromocytomas, multifocal paragangliomas, or biochemically silent disease, yearly imaging is indicated. This may be because of an enchancment in extracellular volume and a lower in rostral fluid accumulation during recumbence/sleep. However, they sometimes come to medical consideration because of different features of the syndrome (weight gain, fatigue, muscle weak spot, pores and skin changes, anxiousness, glucose intolerance, hyperlipidemia, osteopenia) quite than hypertension. Hypertension is seen in ~40% of patients with hypothyroidism and has a predominantly diastolic phenotype associated with elevated systemic vascular resistance and decreased arterial compliance. Because of low cardiac output, patients might have a slim pulse strain regardless of stiff vessels. Hypertension in hyperthyroidism is primarily systolic and is expounded to elevated cardiac output.
Order 25 mg antivert free shippingThe ostia are then opened medicine 832 order 25mg antivert with mastercard, and the posterior wall of the septum is resected to expose the face of the sella my medicine discount antivert 25 mg amex. A related dissection may be used for the contralateral nasal passage to enable for a binostril approach symptoms 6 days post iui buy 25mg antivert visa. The choice to perform a binostril approach is dependent upon the size of the tumor treatment gout order antivert 25 mg otc, the need for extension of the sphenoidotomy, or surgeon desire. Although nonetheless a minimally invasive method, a larger exposure trades the benefit of a wider surgical corridor and viewing window for distortion of the conventional anatomy and nasal function. Once the face of the sphenoid sinus is resected, the encompassing contents are uncovered. The bone of the sella continues superiorly as the tuberculum sellae after which further on anterosuperiorly because the planum sphenoidale. The carotid protuberance may be seen as a bony outpouching that serves to establish the underlying carotid artery because it runs vertically at the skull base on the lateral aspect of the sella. The sellar floor is then penetrated, and the opening is widened utilizing a Kerrison punch. The dura is incised, and an attempt is made to set up a particular cleavage plane between the pituitary gland or tumor and the underlying dura. The potential for getting into the cavernous sinus and encountering important venous bleeding exists when dissecting between these two layers. Internal debulking of the tumor allows for the capsule of the tumor to collapse down onto itself and turn out to be accessible to the surgeon. Finally, numerous angled endoscopes enable the surgeon to inspect the cavity for residual tumor. However, if a tear in the arachnoid is observed, not only does it add to the complexity of the case, but additional steps have to be taken to close the communication between the sinonasal cavity and the intracranial compartment. Sellar reconstruction is carried out by placing the autologous fascia lata and/or fats graft over the dural opening and packing it within the sphenoid sinus. There are numerous strategies for extra closure methods, including the usage of mesh, cartilage, bone, or tailor-made artificial grafts. However, at our institution, a nasoseptal flap, with its accompanying vascular provide from the nasoseptal department of the sphenopalatine artery, is placed over the fats graft to provide a further vascularized layer of safety. For closure of the nasal portion of the process, the septal flaps are reapproximated and the nasal septum is returned to its midline insertion. For instances by which the sphenoid sinus has been full of a graft, small absorbable gelatin sponges could additionally be placed in the sphenoethmoidal recess to buttress the sphenoid packing, and gauze packing is left in place throughout the nasal cavity. The main limitation of the transcranial approaches is that the intrasellar portion of the tumor may be more difficult to access. Perioperative Considerations Key Concepts Prior to surgery, the size and sort of pituitary tumor must be decided. There are essential traits of a pituitary lesion that should be identified prior to surgery. Knowing the size of the lesion and type of lesion will help determine the surgical method after which information the preoperative, perioperative, and postoperative management for the patient. A macroadenoma has a better likelihood of compromising regular pituitary function, which could find yourself in secondary adrenal insufficiency, growth hormone deficiency, hypothyroidism, and hypogonadism. Patients with a craniopharyngioma are much extra likely to develop panhypopituitarism and diabetes insipidus after surgery. Secondary adrenal insufficiency is usually recommended by signs of fatigue, weight loss, weak point, dizziness, and difficulty concentrating. The most necessary assessments to be made preoperatively are the need for glucocorticoid and thyroid hormone substitute as a outcome of the stress of surgery. This helps differentiate between an "incidentaloma" and a real useful microadenoma. The choice concerning perioperative glucocorticoid protection is dependent upon the end result of preoperative screening. The patient ought to receive forty eight hours of perioperative supraphysiological glucocorticoid remedy, which can then be rapidly reduced. A suggested routine can be 50 mg hydrocortisone every eight hours on day 0, 25 mg every eight hours on day 1, and 25 mg in the morning on day 2. Barring any postoperative complications, glucocorticoid supplementation ought to be discontinued after forty eight hours and depending on the daily morning plasma cortisol ranges obtained between postop days 3 and 5. Identifying the type of secretory tumor has an implication on perioperative management. Intubation of a affected person with acromegaly may be troublesome and may necessitate an awake intubation. Postoperatively, patients with acromegaly may have issue respiratory with nasal packing. Acromegalic sufferers commonly have obstructive sleep apnea requiring continuous constructive airway pressure remedy, which is contraindicated after this surgical procedure. As beforehand acknowledged, hormonal status have to be evaluated for each affected person previous to surgical intervention. Both an arterial line and an indwelling urinary catheter are sometimes used throughout these procedures for intraoperative and postoperative assessment. The optic nerve and chiasm are notably delicate to damage, and damage might occur with even minimal quantities of retraction and even with overpacking the sella during sellar reconstruction. Case stories reveal that underpacking of the sella can result in a secondary empty sella with late onset of imaginative and prescient loss because of chiasmatic prolapse, though this event has not been encountered by us. Postoperative Complications Key Concepts Pituitary surgical procedure is associated with a low rate of morbidity/ mortality. Postoperative Management Key Concepts Diabetes insipidus happens in 18% to 31% of patients undergoing pituitary surgical procedure. A 2009 systematic evaluate and metaanalysis particularly centered on endoscopic pituitary surgical procedure outcomes within the literature. It is extraordinarily tough to control brisk arterial blood move when visualization of the operative field is obscured by blood and solely limited devices are available. Suction and tamponade can often provide the visible window essential to management the scenario. Rhinological issues are distinctive to the endonasal approach and occur in roughly 1% to 2% of circumstances. Hyposmia can be seen in the postoperative interval, however this is most often transient. Many of the rhinological problems can be prevented with meticulous and nondestructive surgical method during the exposure. When confronted with diuresis after surgery, it ought to be assumed to be diabetes insipidus until confirmed in any other case. More generally encountered than diabetes insipidus are postoperative diuresis and glucosuria. Fluid intake from the working room should be included in the whole steadiness documented as a result of fluid may have been administered intravenously through the operation.
Buy 25mg antivert overnight deliveryThe American Society of Anesthesiologists developed a follow advisory for prevention of this complication based totally on case series treatment 3rd degree burns 25mg antivert visa, case reviews treatment zoster order 25 mg antivert fast delivery, case-control research medicine in the 1800s buy antivert 25mg without prescription, and skilled opinion symptoms 5 weeks pregnant discount antivert 25 mg without a prescription. Cortical blindness is attributable to embolic phenomenon or profound and prolonged hypotension. Summary Spinal surgeries have increased in number dramatically over the past three a long time. As affected person comorbidities and complexity of surgical interventions increase, so does the need for critical care management of these patients in both the preoperative and postoperative intervals. Rehabilitation and ache administration is usually a main impediment to a smooth postoperative recovery, and consultations with these specialists must be initiated as early as potential. Knowledge of site-specific problems is crucial to the administration of spine surgical procedure patients. Complex backbone surgical procedure is associated with a relatively excessive incidence of prolonged mechanical ventilation or reintubation, notably after anterior cervical backbone surgical procedure. Trends, main medical problems, and charges associated with surgery for lumbar spinal stenosis in older adults. Effects of age and comorbidities on complication charges and adverse outcomes after lumbar laminectomy in elderly patients. Prehabilitation and early rehabilitation after spinal surgical procedure: randomized clinical trial. Costs and quality of life for prehabilitation and early rehabilitation after surgery of the lumbar spine. Prevalence of opioid dependence in backbone surgical procedure sufferers and correlation with length of stay. Strategies in postoperative analgesia in the obese obstructive sleep apnea patient. Abilities of pulse strain variations and stroke volume variations to predict fluid responsiveness in prone position during scoliosis surgical procedure. Responding to neuromonitoring changes in 3-column posterior spinal osteotomies for rigid pediatric spinal deformities. Effect of hemorrhage and hypotension on transcranial motor-evoked potentials in swine. Operative length as an unbiased threat factor for postoperative problems in single-level lumbar fusion: an evaluation of 4588 surgical instances. Clinical review: postextubation laryngeal edema and extubation failure in critically ill adult patients. The use of somatosensory evoked potentials to determine the relationship between patient positioning and impending upper extremity nerve damage during backbone surgery: a retrospective evaluation. Patient elements, comorbidities, and surgical traits that enhance mortality and complication threat after spinal arthrodesis: a prognostic research based on 5,887 patients. Short-term morbidity and mortality related to correction of thoracolumbar mounted sagittal aircraft deformity: a report from the Scoliosis Research Society Morbidity and Mortality Committee. C5 palsy following anterior decompression and spinal fusion for cervical degenerative ailments. Vocal cord palsy following anterior cervical backbone surgery: a qualitative systematic review. Risk elements for postoperative retropharyngeal hematoma after anterior cervical spine surgical procedure. Incidence, outcomes, and mortality of reintubation after anterior cervical fusion. Unstaged versus staged posterior-only thoracolumbar fusions in deformity: a retrospective comparability of perioperative issues. Comparative safety of simultaneous and staged anterior and posterior spinal surgery. The timing of surgical staging has a major impact on the issues and functional outcomes of grownup spinal deformity surgery. Morbidity and mortality associated to odontoid fracture surgical procedure in the elderly inhabitants. Incidence of postoperative symptomatic epidural hematoma in spinal decompression surgical procedure. Risk factors associated with ischemic optic neuropathy after spinal fusion surgical procedure. Practice advisory for perioperative visible loss associated with spine surgery: an up to date report by the American Society of Anesthesiologists Task Force on Perioperative Visual Loss. Otolaryngologic administration of delayed pharyngoesophageal perforation following anterior cervical spine surgery. The incidence of C5 palsy after multilevel cervical decompression procedures: a evaluation of 750 consecutive circumstances. Prospective evaluation of incidence and threat components of dysphagia in backbone surgical procedure sufferers: comparability of anterior cervical, posterior cervical, and lumbar procedures. Factors that correlate with the decision to delay extubation after multilevel inclined spine surgical procedure. Perioperative issues of posterior lumbar decompression and arthrodesis in older adults. Ideally, the anesthesia group ought to have a workstation or physiological monitor in the control room to reduce exposure to radiation during the procedure. Typically, the anesthesiologist is positioned on the other facet of the affected person because the proceduralist, with the anesthesia equipment far off to one facet to minimize interference with movement of kit in the course of the process. Anesthesiologists have to anticipate the logistics referring to this arrangement, together with including extensions to monitoring equipment and intravenous/arterial tubing. The anesthesiologist ought to have the power to observe the affected person and have quick access to the anesthesia machine and tools corresponding to infusion pumps. The anesthesia team should have access to the displays that show real-time fluoroscopy images so as to follow the procedure and anticipate intervals of elevated danger to the patient. Recently increased consideration has been placed on optimizing the design of those suites to decrease radiation exposure to anesthesia staff as properly as the proceduralists, which is usually not the case. Endovascular neuroradiology procedures may be elective, such as an embolization of an unruptured intracranial aneurysm. In contrast, these procedures may be emergent, such as for endovascular remedy of acute ischemic stroke. Factors related to the affected person and procedure will information the decision as to whether or not the patient receives general anesthesia or sedation. Clinical Pearl Anesthesiologists should be capable of follow the procedure so as to anticipate high-risk time durations. These refined spaces utilize biplane digital angiography gear and software program to produce high-resolution and three-dimensional photographs. The use of intravascular distinction dye has several implications for the anesthesiologist. First, these distinction dyes are nephrotoxic and have the potential to cause deterioration of renal function.
Safe antivert 25 mgIt can vary from no effect treatment keloid scars cheap 25 mg antivert free shipping, to a modest decrease in cardiac output medicine man lyrics best 25mg antivert, to a full cardiac arrest medications ok for dogs generic antivert 25 mg otc. The growth of an air lock in the coronary heart and pulmonary artery can make standard resuscitation efforts futile medicine lux discount antivert 25mg amex. One hundred p.c oxygen is run, and concomitantly the neurosurgeons are suggested of the doubtless analysis. If possible, the site of surgical procedure should be brought close to the level of the guts. The main causes are venous occlusion, intraparenchymal hemorrhage, edema of mind tissue associated to underlying disease or intraoperative mind trauma, arterial hypertension,fifty three,fifty four and extreme hypoxemia and hypercapnia. If neurological signs referable to probably air are current, consideration may be given also to artificially increased blood stress and hyperbaric oxygen therapy,50 though no evidence-based pointers could be provided. If surgery needed to be abruptly stopped, then the wound may have been contaminated or not properly closed. Prophylactic antibiotics ought to be thought-about, and when stable, the causes of acute intraoperative brain swelling are summarized next. Several conditions might come up during a craniotomy where venous outflow could also be compromised. During a craniotomy, cytotoxic or vasogenic edema leading to overt tissue swelling might arise from a number of causes. In order to produce or exacerbate brain edema, extracranial elevated venous pressure needs to be significant. When this arises and the cranium is open, the combination of elevated venous strain from coughing with arterial hypertension could cause the mind to swell briefly. However, if it produces herniation of mind by way of the craniotomy, venous occlusion can come up, resulting in intractable edema that will require amputation of herniated brain tissue. Metabolic causes or contributors to cerebral edema and swelling embody hypoxemia, hypercapnia, hyponatremia, and osmolar gradients. The neurosurgeon prevents or attenuates procedure-related mind swelling through consideration to venous drainage of surgical beds and minimizing brain retraction as a lot as feasible. Surgical resection of edematous brain or efficiency of a decompressive craniectomy may be wanted. Metabolic issues are usually beneath the control of the anesthesiologist and require their correction as a major goal. This could imply correction of airway issues, prognosis and administration of gas change issues, avoidance of systemic hypertension, and evaluation and correction of osmolar factors. In any occasion, for all conditions of intraoperative mind swelling, the anesthesia staff might carry out maneuvers to diminish the edema via induction of burst suppression with barbiturates or propofol,67 hyperventilation, treatment of hypoxemia, and administration of hypertonic saline68 or mannitol. As with management of intracranial hypertension, avoidance of hypotension and hypertension can be a element of intraoperative administration of problematic brain edema. Edema arising from ischemia, venous occlusion, or tissue trauma edema might progress. If related to postoperative venous thrombosis,seventy three consideration could additionally be needed for anticoagulation or endovascular clot disruption. If of great dimension, a return to the working room could additionally be essential for decompression and/or clot removal. Intraoperative cardiac arrest arises primarily from iatrogenic, hemorrhagic, embolic, metabolic, medical, or airway-related causes. Iatrogenic causes embody cardiac arrests associated to anesthetic problems/errors75 or surgical errors or misadventures. Excessive blood loss and/or hypovolemia with insufficient alternative will cause progressive hypotension, which might lead to cardiac arrest. Problems associated to organ dysfunction, drug effects, or toxic ingestions might trigger deadly arrhythmias resulting in cardiac arrest. Myocardial supply�demand imbalance in the context of coronary artery disease can predispose to acute myocardial dysfunction and lethal arrhythmia each throughout and after surgery. Severe cardiomyopathy can lead to cardiac arrest probably associated with variations in preload or afterload associated to anesthetics, fluid administration, or hemorrhage. Some severe preexisting cardiac valvular abnormalities may result in cardiac arrest. Most notable is extreme aortic stenosis, which, with decreased intraoperative blood pressure, could result in hypoperfusion of myocardium and consequent refractory cardiac arrest. Airway mishaps are reported to be a major cause of anesthesia morbidity and mortality. Difficulties with extubation are typically related to surprising new airway abnormalities which will interfere with spontaneous or assisted ventilation. Examples include intraoperative extubation while prone or with the top in pins flexed forward or other position associated with tough access to the airway. This could embrace use of extracorporeal support84 or unconventional chest compression methods, for example, two-person front-back compressions used in the lateral position or again compression in the inclined position. Cardiac arrest within the susceptible place typically mandates immediately inserting the patient supine to enable proper chest compressions. The surgeon must effect a fast overlaying of the wound, elimination from head fixation pins if in place, after which turning onto a gurney or mattress introduced rapidly into the operating room. Some have suggested an a priori particular mattress configuration that may quickly facilitate these targets with out removing the pins. Cardiac arrest arising in these positions requires turning the affected person on the operating room bed to the supine place while the 7 Intraoperative Catastrophes seventy nine surgeon quickly covers the wound and controls the head place through the turn. Two-person front-back compressions within the lateral place has been described on this circumstance. Rapid administration of blood products containing citrate can exacerbate the issue through hypocalcemia such that periodic empiric CaCl2 is acceptable and ionized calcium ought to be assessed periodically. Evaluation of correctable issues that will have arisen throughout surgical procedure to trigger the cardiac arrest must be considered and treated: Local anesthetic toxicity could cause a cardiac arrest. Pneumothorax or hemothorax must be thought-about if a central line was positioned or surgery is close to the chest. Major vascular harm of the iliac vessels, vena cava, or aorta ought to be considered when cardiac arrest without apparent trigger arises during spinal surgical procedure. Given the publicity to multiple medicine and latex that can come up during surgical procedure, this is a crucial consideration in evaluating the potential causes of intraoperative cardiac arrest. In the context of out-of-hospital cardiac arrest, data recommend a helpful effect of hypothermia, though there continues to be debate regarding the depth of hypothermia and whether the neuroprotective effect is actually prevention of fever. Moreover, hypothermia might produce problematic coagulopathy, which can produce a postoperative hemorrhage. If intracranial or perispinal, this might negate any possible benefits of the hypothermia. This could also be significantly true within the scenario of refractory bupivacaine toxicity,111 hypothermia,112 massive venous or thrombotic or air embolism,113�115 or other doubtlessly reversible causes.
Cheap 25 mg antivertCalcium channel blockers corresponding to nicardipine and short-acting betablockers like esmolol are sometimes used to actively lower the blood pressure symptoms 6dpo antivert 25mg. However acne natural treatment discount antivert 25 mg line, in the course of the periods of momentary clipping symptoms 32 weeks pregnant cheap antivert 25mg otc, the blood pressure could also be actively raised to ensure blood circulate through the collateral channels to avoid cerebral ischemia medicine 5513 cheap 25 mg antivert with mastercard. Occasionally, in order to facilitate clipping of giant basilar tip aneurysms, intraoperative momentary cardiac standstill is offered using high-dose adenosine (0. Invasive arterial blood stress monitoring is used to titrate hemodynamic objectives throughout craniotomy. Patients present process craniotomy sometimes obtain nonglucose-containing warm, isotonic intravenous fluids. Despite using diuretics to facilitate brain leisure, the objective is to maintain normovolemia through the procedure. Some typical examples include resection of a large arteriovenous malformation or meningioma, intraoperative rupture of an aneurysm, and inadvertent vascular damage. The transfusion triggers for neurosurgical patients are considerably elusive, although traditionally, a hemoglobin stage of 10 g/dL was usually thought of to be a stability between optimal oxygen-carrying capability and rheology of blood to facilitate perfusion of cerebral microvasculature. However, more recently, decrease hemoglobin values have been advocated in neurosurgical patients. Anemia in neurosurgical sufferers is related to poor outcomes, but so is the utilization of transfusion of blood. Although the safety of acute normovolemic hemodilution during craniotomy has been demonstrated,34 the apply has not gained substantial recognition. In addition, brain rest is fascinating to facilitate surgical publicity and mind retraction. Volatile anesthetic brokers are used in low concentrations to avoid direct cerebral vasodilation, and in sufferers where mind swelling is anticipated, intravenous anesthesia with propofol (but avoiding hypotension) is commonly most popular. Selection of acceptable anesthetic agents (intravenous anesthetics for patients with anticipated mind swelling) three. Optimal positioning with slight head elevation and avoiding extreme neck flexion or rotation 4. Intraoperative Monitoring the details of intraoperative neuromonitoring are mentioned in Chapter 6. Evoked potential monitoring and electroencephalography are more and more being used. In addition, monitoring for venous air embolism may embrace transesophageal echocardiography or precordial Doppler. Three p.c hypertonic saline is associated with related brain leisure and arteriovenous oxygen and lactate difference. The quantity of urine output from mannitol- and/or furosemide-induced diuresis is usually replaced with isotonic crystalloid or regular saline. Finally, fever and seizures should be promptly treated, and in refractory circumstances, burst suppression with thiopental or propofol could also be attempted. Temperature Management Key Concept Intraoperative hypothermia should be averted by using forced-air warming blankets, warming intravenous fluids, and adjusting room temperature. Brain leisure utilizing mannitol/furosemide can lead to continued electrolyte imbalance postoperatively and ought to be monitored and corrected aggressively. General anesthesia is associated with a decrease within the physique temperature as a outcome of peripheral vasodilatation and redistribution of the body warmth from the core. Forced-air warming blankets, warmed intravenous fluids, and adjustment of the working room temperature are some strategies used to preserve normothermia underneath anesthesia. Clinical benefits of intraoperative hypothermia in different neurosurgical circumstances have also not been demonstrated. Emergence from General Anesthesia Key Concepts Emergence from craniotomy must be speedy and clean, with minimal hemodynamic modifications and straining on the tracheal tube. Glycemic Management Key Concepts Glucose levels may fluctuate intraoperatively and should be monitored. Given the association of both hypoglycemia and hyperglycemia with poor outcomes in neurosurgical patients, the aim of anesthetic administration is to keep normoglycemia. The surgical stress response and perioperative steroid use typically contribute to intraoperative hyperglycemia. In truth, new-onset intraoperative hyperglycemia could also be observed during craniotomy in patients who had normal blood glucose levels preoperatively. The goal for emergence from anesthesia for craniotomy is to have an awake patient in order that a neurological examination may be performed reliably. Patients who were intubated preoperatively, these with poor neurological standing, and sufferers undergoing extended surgery across the brainstem are likely to remain intubated. Emergence from anesthesia requires diligent planning to accomplish a timely, easy emergence with minimal hemodynamic perturbation and straining on the tracheal tube. Anesthetic agents are steadily weaned, and the patients are trialed on spontaneous air flow to decide if their respiratory drive and minute ventilation are applicable. With the trendy short-acting anesthetic brokers, speedy emergence could be completed in most cases. Incorporation of dexmedetomidine within the anesthetic regimen is one other strategy to facilitate shorter emergence and restoration time in neurosurgical patients45 with attenuation of delirium, and scalp blocks have been proven to enhance restoration profiles. The adrenergic surge related to emergence could also be handled with a short-acting opioid or an antihypertensive corresponding to esmolol or nicardipine. Coughing and straining on the tracheal tube during emergence could be prevented with lidocaine or even handed use of remifentanil. Perioperative hypertension has been related to increased incidence in postoperative intracranial hemorrhage in sufferers undergoing craniotomy and should be averted. Clinical Pearl Patients should virtually never be extubated beneath deep anesthesia after craniotomy. Extubation should be easy and without hemodynamic response with a affected person who can yield a valid neurological examination. Immediate Postoperative Management Key Concepts Opioids are the mainstay of postcraniotomy ache control but should be used judiciously to avoid respiratory and neurological despair. Data on the impact of craniotomy site on the severity of ache are somewhat conflicting. Regional scalp blocks attenuate the postcraniotomy ache and stress responses however appear to remain underutilized. Although the revealed randomized managed trials of regional scalp block are small and of restricted methodological quality, metaanalysis exhibits lowered postoperative ache. Ondansetron four mg given on the time of dural closure is protected and efficient in preventing emetic episodes after elective craniotomy. Granisetron 1 mg supplies comparable prevention of emesis after supratentorial craniotomy. Some frequent indications for reintubation are neurological deterioration, respiratory distress, copious oropharyngeal secretions, and seizures.
Buy 25mg antivertIt offers antiidiotypic antibodies 25 medications to know for nclex generic antivert 25mg, reduces the expression and function of Fc receptors on leukocytes and endothelial cells medicine 230 25mg antivert overnight delivery, will increase IgG clearance shakira medicine purchase antivert 25 mg on-line, downregulates the activation and effector operate of T and B cells medicine in the 1800s cheap 25mg antivert with mastercard, and inhibits complement activation and cytokine production. The normal dose is 2 g/kg as much as a maximum of 140 g in a single administration infused over four to eight hours. Minor reactions, such as flushing, chills, headache, nausea, myalgia, and arthralgia, are common; these are decreased with premedication and by slowing the infusion rate. Acute kidney harm, because of osmotic nephrosis from the sucrose or sorbitol vehicle, is often self-limited. Proteasomal inhibition results in the buildup of misfolded IgG and causes apoptosis of plasma cells. The major toxicity of bortezomib is neurologic, with de novo or worsened peripheral neuropathy being widespread. Carfilzomib (Kyprolis) is a second-generation proteasome inhibitor that irreversibly binds to and inhibits the chymotrypsin-like activity of the 20S proteasome. A section I clinical trial of carfilzomib as part of a desensitization technique in kidney transplant candidates is currently underneath means. Eculizumab (Soliris) is a monoclonal antibody to the complement protein C5, which blocks C5 cleavage and halts the formation of the membrane assault advanced. Because eculizumab diminishes the protection towards encapsulated micro organism, especially meningococci, sufferers ought to ideally bear meningococcal vaccination earlier than receiving the first eculizumab therapy. After the acute rejection episode has been handled, intensification of the maintenance routine and closer monitoring are often indicated. Treatment of acute cellular rejection requires using brokers directed towards activated T cells. Steroids reverse about 75% of first acute rejections and are sometimes tapered down over a few weeks to upkeep doses of 5 to 10 mg/day. The management of persistent allograft rejection is troublesome as a result of the histologic modifications seen are often irreversible and result in the development of kidney illness, whatever the original harm. The risks and advantages of immunosuppression should be weighed carefully at each stage. If graft perform continues to deteriorate, immunosuppression must be withdrawn in a stepwise style to avoid precipitating acute rejection, and the affected person must be prepared for dialysis, preemptive transplant, or complete conservative care. In addition, the recipient should be succesful of reply usually to immune stimuli, such as infection and tumors. Transplant tolerance is therefore an active state of antigen-specific nonresponsiveness, quite than a failure to reply to the allograft. Upon reconstitution of immune function, the recipient not acknowledges new antigens offered during a important period as nonself. Early animal studies confirmed that fetal/ neonatal publicity to donor blood cells led to hematopoietic chimerism and particular transplant tolerance. In the precyclosporine era, improved kidney transplant outcomes had been seen with donor-specific blood transfusions. These disappeared after the introduction of CsA, presumably as a result of the efficacy of this drug in blocking T cell activation. Several mixtures of biologics can be envisioned as probably inducing tolerance. Regulatory T cells (Tregs) were discovered to suppress the rejection response of naive T cells in adoptive switch assays. Several studies involving the use of Tregs in kidney transplant recipients as both tolerogenic agents or immunotherapy for graft inflammation are presently beneath method. The improvement of new brokers and improved understanding of transplant immunology are now allowing us to create simplified immunosuppressive regimens with low toxicities which have the potential to enhance long-term patient and graft survival. These strategies have limited sensitivity and specificity for the prognosis of rejection, which is normally made by kidney biopsy. Biomarkers may serve not solely as diagnostic parameters but also as predictive tools that anticipate the next development of subclinical and clinical acute rejection. The identification of biomarkers of immune alloreactivity in blood, urine, and tissue would enable the early identification of patients in danger for rejection, the optimization of drug regimens, and the monitoring of responses to adjustments in remedy and would guide the event of novel therapies. Studies in human kidney recipients suggest unique protein and genetic signatures that may establish biomarkers of injury as properly as potential targets of remedy. It is much less particular, and modifications in check values may be extra predictive than single time point assessments. A widespread rejection module consisting of eleven genes which may be considerably overexpressed in acute rejection was initially identified in 4 several types of transplanted organs. It is now being developed as a urinary biomarker to establish kidney transplant recipients with subclinical rejection. Tacrolimus enhances remodeling development factor-beta1 expression and promotes tumor progression. Interleukin-2-receptor blockade with daclizumab to prevent acute rejection in renal transplantation. A randomized, multicenter study of steroid avoidance, early steroid withdrawal or commonplace steroid therapy in kidney transplant recipients. The growth of dependable biomarkers is crucial for individualizing remedy aimed toward extending allograft survival and bettering patient health, significantly when incorporating novel immunosuppressive agents, implementing drug minimization protocols, and selecting patients for transplant tolerance trials. Rapamycin inhibits the growth and metastatic progression of non-small cell lung cancer. Transplant glomerulopathy: subclinical incidence and association with alloantibody. Conversion to sirolimus for chronic renal allograft dysfunction: danger components for graft loss and severe unwanted effects. Clinical advantages of Neoral C2 monitoring within the long-term administration of renal transplant recipients. Bortezomib provides efficient remedy for antibody- and cell-mediated acute rejection. Immunosuppression with belatacept-based, corticosteroid-avoiding regimens in de novo kidney transplant recipients. Evidence for antibody-mediated damage as a serious determinant of late kidney allograft failure. Mycophenolate mofetil decreases acute rejection and may improve graft survival in renal transplant recipients when compared with azathioprine: a scientific evaluation. Efficacy and safety of tacrolimus compared with ciclosporin A in renal transplantation: threeyear observational outcomes. The antigen-specific, main histocompatibility complex-restricted receptor on T cells. A prospective, randomized trial of tacrolimus in combination with sirolimus or mycophenolate mofetil in kidney transplantation: results at one year. Mycophenolate mofetil reduces late renal allograft loss unbiased of acute rejection.
References - Tak ECPM, van Hespen A, van Dommelen P, et al: Does improved functional performance help to reduce urinary incontinence in institutionalized older women? A multicenter randomized clinical trial, BMC Geriatr 12:51, 2012.
- Raz R: Asymptomatic bacteriuria: clinical significance and management, Int J Antimicrob Agents 22:45-47, 2003.
- Vernez SL, Okhunov Z, Kaler K, et al: Skin-to-tumor distance predicts treatment failure of T1A renal cell carcinoma following percutaneous cryoablation, Urology 108:195n200, 2017.
- Sinha A, Avery P, Turner S, Bailey S, Cheetham T. Vitamin D status in pediatric patients with cancer. Pediatr Blood Cancer 2011;57:594-598.
- Li Q, Keung EC: Effects of myocardial hypertrophy on transient outward current, Am J Physiol 266:H1738-H1745, 1994.
|