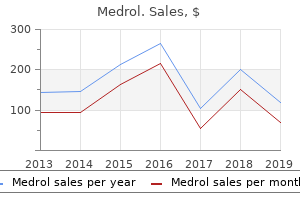
Medrol
Marc E. Stone, MD - Associate Professor of Anesthesiology
- Program Director, Fellowship in Cardiothoracic Anesthesiology
- Mount Sinai School of Medicine
- New York, New York
Buy discount medrol 4mg on-lineCellular Whorls Meningothelial-Like Clusters (Left) Cellular how to treat arthritis in dogs uk discount 4 mg medrol visa, tightly whorled clusters of spindled cells may sometimes be seen in delicate tissue perineurioma rheumatoid arthritis shoulder buy 16 mg medrol fast delivery, considerably harking again to meningioma arthritis pain video purchase medrol 4mg line. Ectopic meningioma tends to occur in areas totally different from perineurioma arthritis glucosamine buy medrol 16 mg free shipping, nonetheless. The elongated, fantastic, cytoplasmic processes of the lesional perineurial cells are nicely evident in this case. Sclerosing Perineurioma Sclerosing Perineurioma (Left) this example of sclerosing perineurioma exhibits scattered lesional cells with round, pale nuclei. Rare Plexiform Perineurioma Intraneural Perineurioma (Left) Rare cases of plexiform perineurioma have been reported. This case arose on the decrease lip of a 60-year-old girl, and exhibits the unique multinodular and serpentine progress sample. Their incidence is likely underestimated given their morphologic overlap with pure nerve sheath tumors. It typically resembles perineurioma architecturally but contains an admixed Schwann cell element. Kacerovska D et al: Hybrid peripheral nerve sheath tumors, including a malignant variant in sort 1 neurofibromatosis. Myxocollagenous Stroma Myxocollagenous Stroma (Left) Some cases of hybrid nerve sheath tumor are extensively myxoid and will histologically and clinically mimic a myxoma. Diffuse Myxoid Stroma Neurofibroma-Like Areas (Left) Areas of hybrid nerve sheath tumor may resemble neurofibroma, significantly when small, separated collagen fibers are present, as depicted in this image. Of notice, some instances of those particular tumors could also be associated with neurofibromatosis or schwannomatosis. Most circumstances are dermal or subcutaneous, and some might prolong immediately up underneath the overlying epidermis. Nuclei are generally small and could additionally be dark with dense chromatin or vesicular with a small nucleolus. Battistella M et al: Vascular invasion and other invasive options in granular cell tumours of the pores and skin: a multicentre research of 119 circumstances. However, to the unwary, this finding may recommend perineural invasion by a malignant process. This picture reveals a subtle tumor cell infiltrate with out the basic overlying marked epidermal changes. It is usually centered inside the dermis and can involve the underlying subcutis as properly. Dermal Papule Schwann Cells (Left) the cells in dermal nerve sheath myxoma have schwannian differentiation. They have uniform spindleshaped or oval nuclei, evenly distributed chromatin, and lengthy fibrillary cytoplasmic processes forming bipolar and stellate configurations. This immunohistochemically stained part depicts diffuse and intense nuclear and cytoplasmic reactivity. Sheth S et al: Differential gene expression profiles of neurothekeomas and nerve sheath myxomas by microarray analysis. A main component of the advanced of myxomas, spotty pigmentation, and endocrine overactivity. Fibrous Septa Thick Fibrous Septum (Left) this medium-power view of a dermal nerve sheath myxoma depicts a thick fibrous septum composed of dense, mature collagen in between myxoid lobules. Although hardly ever seen in dermal nerve sheath myxomas, they supply further proof of schwannian differentiation. Verocay-Like Body Syncytial Nests and Vacuoles (Left) the neoplastic cells of nerve sheath myxoma include spindle and epithelioid cells with uniform, bland, oval, and elongated nuclei and abundant eosinophilic cytoplasm. They are regularly organized in syncytial nests and sometimes have intracytoplasmic vacuoles as depicted. Ring-Like Structures 540 Dermal Nerve Sheath Myxoma Peripheral Nerve Sheath Tumors Papule Cohesive Structures (Left) this scanning-power micrograph depicts a dermal nerve sheath myxoma with a raised, exophytic sample because of an expansile myxoid lobule in the superficial dermis. Reticulated Pattern Multilobular and Plexiform Architecture (Left) this micrograph exhibits bipolar and stellate spindle cells in a dermal nerve sheath myxoma, with abundant eosinophilic cytoplasm and long, interconnecting cell processes, forming a reticulated or community sample. In the latter location, the tumor could additionally be extraadrenal (shown) or intraadrenal (much less common). Ganglioneuroma Features Schwannian Stroma (Left) the stroma of ganglioneuroma is composed of mature Schwann cells with typical neural cytologic options (elongated nuclei with tapered or pointed ends) inside a collagenous and variably edematous background. Hu J et al: Retroperitoneal composite pheochromocytoma-ganglioneuroma: a case report and evaluation of literature. Intracytoplasmic Pigment Size Variation (Left) Ganglion cells differ extensively in measurement from tumor to tumor, and the cytoplasm ranges from pale to deeply eosinophilic. Large Clusters or Nests Fascicle Formation (Left) the lesional cells of ganglioneuroma may be more compact and bundled in areas, resembling irregular nerve fibers. Fascicle Formation (Cross Section) 544 Ganglioneuroma Peripheral Nerve Sheath Tumors Cellular Fascicles Myxoid Stroma (Left) Some instances of ganglioneuroma comprise more mobile, fascicular foci. Myxoid Stromal Change Mild Degenerative Atypia (Left) this image shows a myxoid focus of ganglioneuroma by which the lesional cells are individually separated from one another quite than in bundles. Fat is extra prone to be present close to the periphery the place the tumor interfaces with surrounding gentle tissue. It can also be seen in ganglioneuroblastoma, and subsequently an intensive seek for neuroblastic elements is warranted in these instances. Whorls and Nodules Infiltrative Growth (Left) Ectopic meningioma sometimes shows infiltrative development throughout the surrounding gentle tissues, as proof on this picture by the admixed collagen bundles and mature adipose tissue. Histologically, it exhibits collagenous stroma with slit-like vascular areas lined by meningothelial cells. Mature Glial Tissue Fine Fibrillary Matrix (Left) Mature glial tissue is evidenced by the presence of astrocytes and different cells lightly distributed inside a fantastic fibrillary matrix. It is indistinguishable from main fibromatosis consisting of fascicles of bland myofibroblasts and fibrous stroma. Tumor cells are spindled to epithelioid and related to a extremely variable amount of melanin pigment. Nuclear palisading could also be seen in occasional instances however is normally much much less outstanding as compared to conventional schwannoma. Cells with cytoplasmic vacuolization can also be seen in some instances and can mimic adipose tissue when prominent. This case confirmed areas of in depth pigmentation that obscured underlying cytologic features. Torres-Mora J et al: Malignant melanotic schwannian tumor: a clinicopathologic, immunohistochemical, and gene expression profiling research of forty circumstances, with a proposal for the reclassification of "melanotic schwannoma". In these conditions, a common finding is the preservation of tumor cells solely around vessels (peritheliomatous pattern) with necrosis of the intervening cells. Demonstration of origin from a nerve or benign nerve sheath tumor (mainly neurofibroma) may be very helpful. Diffuse S100 expression is usually very uncommon and may elevate the potential of melanoma or mobile schwannoma. The glands might or may not present proof of mucin production and can typically show focal neuroendocrine differentiation. Some vessels, nonetheless, lack this modification, and others could appear more dilated or even "staghorn.
Medrol 16 mg saleThe frequent issues talked about are bleeding arthritis in neck heat or cold quality medrol 4 mg, infection arthritis in the knee medication buy medrol 4mg amex, and pancreatic fistula arthritis in knee fluid medrol 16 mg low price. However reversing arthritis in neck cheap medrol 16 mg without a prescription, percutaneous or endoscopic aspiration has the potential to spill malignant cells into the peritoneum with subsequent seeding and lowered survival. In the absence of an excellent radiologic or pathologic check to determine the analysis preoperatively, medical characteristics such as age, gender, and the presence of signs could also be helpful within the choice to function. Surgical Approach A full resection of the cystic lesion is essential to stop recurrence or subsequent manifestation of malignant disease. The venous collaterals in the splenic hilum are suture ligated after dissection of the pancreatic tail. The splenic vein is ligated on the level of pancreatic transection 2 cm from the lesion, preserving the inferior mesenteric vein. The cyst wall is hyalinized and focally calcified, and the cavity incorporates plentiful mucin, according to a analysis of benign mucinous cystic neoplasm. In this occasion, the affected person is tolerating the fistula properly, and a bag without suction may be related to drain residual fluid with nursing recommendation before discharge house. Case Continued the patient has minimal elevation of her serum amylase on the primary postoperative day. She continues to make good progress and advances to full liquids by postoperative day four and a low-fat food regimen by postoperative day 5. Despite this increase in drain amylase, the drain output is low and averages 60 mL per day. She continues to enhance, is ambulating by postoperative day 9, and is discharged residence with the drain in situ. The drain output continues to decrease steadily, and at follow-up in clinic three weeks later, the drain is removed with no additional problems. Discussion the morbidity of a "pure" pancreatic fistula is lower than that of a fistula from a pancreatic-enteric anastomosis. In this setting, octreotide is usually not needed, and stenting of the pancreatic duct could cause more bother by introducing micro organism from the duodenum and inflicting a stricture. Case Continued At present, four years postsurgery, the patient is doing properly and is symptom free. Discussion nearly all of benign cystic neoplasms of the pancreas are serous cystadenomas, whereas strong and cystic papillary (Hamoudi) tumors are quite rare. These benign lesions regularly can become fairly giant and symptomatic, ultimately requiring a serious pancreatic resection, whereas early intervention would possibly allow enucleation or restricted resection. In sufferers with mucinous cystic neoplasms, cystic neuroendocrine tumors, and benign intraductal papillary mucinous neoplasms, early surgery will forestall malignant degeneration and is likely to be less expensive than statement. Thus, surgical excision is really helpful for pancreatic cysts that increase underneath observation, are symptomatic, and are discovered in healthy older sufferers. For cystic tumors within the tail of the pancreas, resection stays the operation of selection. Splenic preservation ought to be strongly considered in patients suspected to have a benign or premalignant lesion in the pancreatic tail. For small cystic tumors within the uncinate, head, neck, and physique of the pancreas, enucleation might have advantages over pancreatic resection with respect to operative time, blood loss, and preservation of pancreatic parenchyma. Because the pancreas is in any other case regular in these patients, the danger of pancreatic fistula is excessive. However, the morbidity of a "pure" pancreatic fistula that will occur after an enucleation is usually lower than that of a fistula from a pancreatic-enteric anastomosis after a pancreatoduodenectomy. Clinical evaluation in contrast with cyst fluid analysis within the differential prognosis of cystic lesions within the pancreas. The patient is without any complaints, together with nipple discharge, pores and skin changes, tenderness, or palpable mass. The patient is gravida 2, para 1, abortion 1, with her first childbirth at age 35. The supraclavicular, axillary, and cervical regions are free of serious lymphadenopathy bilaterally. A new group of clustered fantastic, linear, heterogeneous, and punctuate calcifications is seen in the lower outer quadrant of the best breast. Mammograms Differential Diagnosis the differential diagnosis for mammographic calcifications includes fibrocystic ailments, true mineral deposits, milk of calcium (calcium within the fluid of a noncancerous cyst), inflammation (mastitis), fibroadenomas, and cancer. In this affected person with clustered fine, linear, heterogeneous, and punctuate calcifications, an additional diagnostic mammogram of the proper breast is needed, together with magnified views. Discussion Mammography stays the best technique of detection for early breast most cancers. Calcifications in the breast are widespread, and most breast calcifications are benign. However, sure patterns or appearances of calcifications can be associated with cancer and further workup is needed to rule out malignancy. Thus, the recommendation of proper segmental mastectomy with sentinel lymph node biopsy with preoperative mammographic localization is made to the affected person. The risks and issues of the operation, together with breast edema, scar, breast deformity, retained tumor, paresthesias, lymphedema, weak spot, bleeding, an infection, hematoma, discoloration of pores and skin from isosulfan blue dye, allergy to the dye, and even (rarely) more critical complications, are discussed with the affected person. Core biopsy is the process of choice for the biopsy of a nonpalpable mammographic abnormality. Specimen Photograph Surgical Approach the patient has a nonpalpable cancer in the proper decrease outer quadrant and requires preoperative mammographic localization, which is performed by a mammographer. It is important to evaluation the films prior to starting the surgical procedure to determine on the location of the incision and relation of the tumor to the localizing needle. After induction of general anesthesia, 5 mL of isosulfan blue dye is injected across the primary tumor site in the proper lower outer quadrant. After 5 minutes of light therapeutic massage to distribute the dye, a transverse incision is made within the axilla. The complete section of the breast containing the cancer is resected with a rim of 1 to 2 cm of normal tissue. Specimen mammography is obtained to affirm the retrieval of the calcification and clip. Any abnormality on chest xray may be evaluated with computed tomography scan of the chest. In the United States, the overall lifetime risk for the development of breast cancer in women is one in eight. After the prognosis of breast cancer, the scientific stage of the illness must be decided. Breast most cancers is staged based on the dimensions of the primary tumor, the standing of lymph nodes, and the presence of metastases. During the 20th century, the therapy of breast most cancers was modified to enhance practical and cosmetic results.
Medrol: 16 mg, 4 mg
Cheap 16mg medrol with amexLesional myoepithelial cells are arranged in a wide range of patterns arthritis in knee youtube generic medrol 16mg on line, including cords or trabeculae arthritis medication for eczema medrol 16mg on line, just like rheumatoid arthritis life expectancy age trusted 16mg medrol predominantly myxoid examples arthritis surgery purchase medrol 4 mg mastercard. Hyalinized Stroma Pseudovascular Spaces (Left) In some hyalinized myoepitheliomas, irregular nests and cords of cells show central mobile loss or dyscohesion resembling vascular spaces. Aggregates of Clear Cells 654 Myoepithelioma of Soft Tissue Tumors of Uncertain Differentiation Storiform Architecture Hypocellularity (Left) Spindled myoepithelial cells in a collagenous stroma might sometimes undertake a free storiform architecture. Scattered cords and small aggregates of neoplastic myoepithelial cells are evident in scattered patches. Osteoid-Like Hyalinization Sclerotic Matrix (Left) this gentle tissue myoepithelioma reveals unfastened aggregates of plasmacytoid myoepithelial cells inside a dense osteoid-like sclerotic matrix reminiscent of osteosarcoma. Myoepithelial Immunophenotype Rare Osteoclast-Like Giant Cells (Left) Osteoclast-like big cells are a really rare finding in soft tissue myoepithelioma. A metastatic carcinoma from a visceral site must be totally excluded on this situation. These tumors are generally referred to as "parachordoma," but are currently thought-about a morphologic variant of myoepithelioma. In contrast, diffuse nuclear atypia, particularly with outstanding nucleoli, correlates well. Malignant Myoepithelioma Malignant Myoepithelioma (Left) this malignant myoepithelioma with a predominant plasmacytoid morphology exhibits distinguished nucleoli imparting a rhabdoid look. Malignant Myoepithelioma Malignant Myoepithelioma (Left) Malignant forms of myoepithelioma are sometimes more cellular than benign types, and the mitotic fee is usually elevated. A characteristic finding is variable-sized deposits of amorphous, flippantly basophilic calcification. The cut floor varies from tan to white or pink and may show focal hemorrhage or cystic change. Sheet-like or fascicular progress is typical of this kind, and the cells are at all times cytologically uniform. In some instances, fascicles are well-formed and fairly distinguished and may even present a focal "herringbone" sample of progress, as demonstrated on this picture. Some areas are hypocellular secondary to stromal edema, myxoid change, or fibrosis. Variably conspicuous irregular, thin collagen fibers are often described as "wiry" but can appear as thicker bundles. However, this morphology is rather more frequent following radiation therapy or chemotherapy. The cellularity of this variant is usually less than usual, and may subsequently could additionally be doubtlessly misdiagnosed as a benign neoplasm. Identification of areas of more typical morphology or utilization of ancillary studies could be very useful. On biopsy, this look can lead to confusion with lowgrade fibromyxoid sarcoma or myxofibrosarcoma. Notably, in poorly differentiated types with a round cell morphology, membranous expression of this antigen can lead to consideration of Ewing sarcoma. Given the additional characteristic of elongated and wavy nuclei, as seen on this image, a tumor of neural origin could additionally be thought of. In occasional tumors, the presence of extravasated purple blood cells amongst uniform spindled cells can impart an look considerably reminiscent of Kaposi sarcoma. The conventional spindled part is actually all the time current however may be extraordinarily focal. Also notice the cytologic options of the epithelial part: Round to oval nuclei without vital pleomorphism. Overlying ulceration, although not shown right here, may be current, and can lead to medical misdiagnosis as an an infection or chronic reactive process. Admixed small spindled cells may also be recognized and infrequently seem extra conspicuous at the periphery of a nodule. Note that some cells are compressed and appear to have darker cytoplasm and extra hyperchromatic nuclei. Occasionally, this morphology is extra prominent and a vague storiform or fascicular progress sample may be seen. Small nests and cords of cells within fibrotic connective tissue, as depicted, can mimic infiltrating carcinoma. Entrapped tumor cells may appear singly or as irregular clusters, aggregates, or cords. Vesicular nuclei with distinguished macronucleoli are attribute of this variant and help in its histologic recognition. In some instances, the comparatively bland cytologic options might result in tumor cells getting overlooked. It is characteristically compartmentalized, with variably thick fibrous septa dividing and subdividing lobules of tumor cells. Conspicuous delicate, thinwalled vascular channels are widespread and sometimes readily obvious. This morphology could be identified at least focally generally and will typically be intensive. Intracytoplasmic Crystals Solid Growth (Left) In the minority of instances, the nested development is much less conspicuous or seemingly absent, imparting a solid morphology. This sample is particularly widespread in infants and youngsters in the head and neck region. This strong progress pattern may lead to diagnostic confusion with different entities such as melanoma. Some circumstances may contain the dermis, as depicted, resulting in potential misdiagnosis as melanoma. Wreath-like multinucleated tumor large cells with similar nuclear options are additionally a typical finding in clear cell sarcoma. Hocar O et al: Clear cell sarcoma (malignant melanoma) of soppy elements: a clinicopathologic research of fifty two circumstances. Yang L et al: Identification of biomarkers to distinguish clear cell sarcoma from malignant melanoma. Hisaoka M et al: Clear cell sarcoma of soppy tissue: a clinicopathologic, immunohistochemical, and molecular analysis of 33 cases. The intervening fibrous septa are sometimes skinny and delicate as an alternative of thick and sclerotic. Fascicular Growth Eosinophilic Cytoplasm (Left) When reduce longitudinally, the tumor cells have a extra spindled appearance and are organized in long fascicles. Wreath-like multinucleated tumor big cells are also seen and are a helpful diagnostic feature of this tumor. They are arranged in bundles and fascicles and present variable eosinophilic to clear cytoplasm. Note that the cytoplasm typically varies from eosinophilic to clear and may present "frayed" high quality that has been described as "stringy" or "moth-eaten.
Buy generic medrol 16mgHistologic components affecting prognosis following hepatectomy for intrahepatic cholangiocarcinoma arthritis knee treatment ice generic 4 mg medrol amex. Approximately 15 cm distal to the choledochojejunostomy rheumatoid arthritis breast cancer buy medrol 4mg with mastercard, the gastrojejunostomy or duodenojejunostomy is carried out arthritis pain in hip 4 mg medrol with visa. Drains are placed adjacent to the pancreaticojejunostomy and choledochojejunostomy to drain potential anastomotic leaks arthritis in the fingers remedies purchase medrol 4 mg on-line. Other pancreatic neoplasms, similar to cystic neoplasms or islet cell tumors, can also uncommonly current with jaundice. The medical scenario introduced is traditional for most cancers of the pinnacle of the pancreas. Endoscopic ultrasound can be used to additional assess the native extent of disease (vascular invasion, lymph node involvement) and can efficiently acquire a cytologic diagnosis by fine-needle aspiration in a high percentage of patients. Discussion the survival following pancreaticoduodenectomy for periampullary carcinoma is very depending on the location of origin of the primary tumor. Other elements influencing survival embrace tumor differentiation, node standing, and margin standing. The function of adjuvant therapy following resection for pancreatic carcinoma is considerably controversial. In the United States, most centers make use of postoperative chemoradiation, although current European outcomes query the good factor about radiation. Diagnosis and Recommendation this affected person has probably resectable pancreatic carcinoma. She should endure acceptable preoperative medical evaluation in preparation for pancreaticoduodenectomy. Case Continued At laparotomy, the tumor is discovered to be unresectable as a outcome of local invasion of the superior mesenteric vein. Surgical Approach If thorough exploration at laparotomy (or laparoscopy) reveals that the tumor is curable, the next step is to determine whether or not the primary tumor is resectable. After a large Kocher maneuver, the proper gastroepiploic vein and the gastroduodenal artery are divided, and if essential, the common hepatic duct may additionally be transected to obtain entry to the anterior surface of the portal vein. The surgeon ought to perform careful digital examination to exclude encroachment of the tumor to the main regional vessels (portal vein, superior mesenteric vein, and artery). In the absence of such regional invasion, a pancreaticoduodenectomy must be carried out. Either the traditional process or the pylorus-preserving modification is an appropriate possibility. After resection is complete, frozen sections of the margins of the bile duct, pancreatic physique, and uncinate course of ought to be obtained. A Surgical Approach Patients discovered to be unresectable at laparotomy ought to bear operative palliation, which includes hepaticojejunostomy, gastrojejunostomy, and chemical splanchnicectomy. However, if a affected person is found to be unresectable at the time of laparotomy, surgical palliation should be thought-about. Operative palliation ought to include bypass of the biliary tree, often by hepaticojejunostomy. Level I published evidence has proven the efficiency of a prophylactic gastrojejunostomy prevents the event of late duodenal obstruction with growing perioperative issues. Outcome after pancreaticoduodenectomy for periampullary cancer: an analysis from the Veterans Affairs National Surgical Quality Improvement Program. Is prophylactic gastrojejunostomy indicated for unresectable periampullary cancer Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic most cancers: a randomized managed trial. She denies any prior gastrointestinal or constitutional symptoms such as stomach ache, nausea, vomiting, early satiety, diarrhea, constipation, anorexia, or weight reduction. On belly examination, no organomegaly, masses, tenderness, or ascites are famous. Differential Diagnosis the differential diagnosis of a affected person with a cystic pancreatic lesion contains pseudocyst, serous cystadenoma, mucinous cystic neoplasm, intraductal papillary mucinous neoplasm, cystic islet cell tumor, stable and cystic papillary (Hamoudi) tumor, and mucinous cystadenocarcinoma. In the absence of pancreatitis, which otherwise would possibly counsel a pseudocyst, benign lesions include serous cystadenoma and strong and cystic papillary (Hamoudi) tumors. Mucinous cystic neoplasms, intraductal papillary mucinous neoplasms, and cystic islet cell tumors are premalignant or malignant, whereas mucinous cystadenocarcinomas are malignant. A recent evaluation from our establishment (Medical College of Wisconsin) has shown that symptoms and age are predictors of neoplasia. The absence of gallstones on ultrasound, no prior historical past of alcoholic pancreatitis, and the calcifications make a pseudocyst unlikely. Although this affected person is asymptomatic, her age (63 years) raises concerns a couple of premalignant or malignant cystic tumor. The commonest cystic lesions of the pancreas are pseudocysts, which normally are the results of gallstone-induced or alcohol-induced pancreatitis or trauma. Cystic pancreatic neoplasms occur at a median age of fifty to 60 years and with a female:male predominance of 9:1. Symptoms generally encountered are imprecise, nonspecific belly pain, early satiety, nausea, and vomiting. In many sufferers no signs are evident, and lesions are initially recognized as an incidental discovering, as within the case being offered. The remainder of the pancreas is sonographically regular with no pancreatic duct dilatation. Diagnosis and Recommendation the preoperative diagnosis is mucinous cystic neoplasm. The affected person is offered distal pancreatectomy that might be performed by laparotomy. After a 25-year follow-up, there was no significant difference among the many three teams of women with negative nodes or between the 2 groups of girls with optimistic nodes with respect to diseasefree survival, relapse-free survival, distant-diseasefree survival, or general survival. After a 20-year follow-up, there have been no statistically important differences between the 2 groups in contralateral breast most cancers, distant metastases, second main cancer, or overall survival. Thus, adjuvant radiation after breast-conserving remedy is crucial for acquiring local recurrence rates equal to those obtained by mastectomy. However, with elevated screening by mammography, the scale of breast cancers and concomitant nodal involvement have been reducing. This has led to questioning the worth of routine axillary dissection in sufferers with early invasive breast most cancers, as a result of most girls have tumor-free nodes and derive no benefit from their elimination. Sentinel lymphadenectomy is a minimally invasive process that accurately stages sufferers by removing the one or two sentinel nodes which may be most likely to include tumor if metastasis has occurred. It has been proven that if the sentinel node is free of tumor, then this predicts with great accuracy that the relaxation of the axillary nodes are more probably to be free of tumor. Twenty-five yr follow-up of a randomized trial evaluating radial mastectomy, total mastectomy, and total mastectomy adopted by irradiation. Prospective observational study of sentinel lymphadenectomy without further axillary dissection in sufferers with sentinel node-negative breast cancer.
Generic medrol 16 mg with mastercardThe physiologic analysis of patients with lung cancer being thought-about for resectional remedy rheumatoid arthritis vitamins order medrol 4mg amex. A comparative analysis of positron emission tomography and mediastinoscopy in staging non-small cell lung cancer arthritis medication chondroitin discount 4mg medrol amex. She has famous rising shortness of breath and cough for 6 weeks definition of arthritis pdf cheap medrol 16mg without a prescription, however no hemoptysis different types of arthritis in fingers cheap medrol 16mg without prescription. She stop work three weeks in the past due to increasing fatigue, and she or he has misplaced 8 pounds during the last month. The signs of cough and shortness of breath recommend airway compression, and thus recommend lung cancer versus a primary mediastinal tumor or a pleural course of. The scientific findings and the radiographic traits usually enable a presumptive prognosis to be made, and moreover, often outline which checks are wanted for further workup with regard to analysis and staging. Specifically, she denies any neurological symptoms corresponding to headaches or focal weak point, and has no new bone or joint pains. Past medical history, family historical past, social history, and evaluate of methods are unremarkable except for smoking and that her father died of lung cancer. Regional and mediastinal lymphadenopathy are present within the vast majority of sufferers. Differential Diagnosis Continued the mixture of risk factors and the radiographic appearance go away no real doubt that it is a lung cancer. The epicenter of this tumor is in the left lung, though it extends dramatically into the middle mediastinum. Although mediastinal germ cell tumors are more widespread in youthful sufferers, they do occur on this age group and could additionally be rapidly rising. Lymphoma may also exhibit speedy development, however that presentation is more frequent in the pediatric inhabitants and younger adults. Case Continued the affected person undergoes bronchoscopy, which reveals abnormal endobronchial tissue in the left upper lobe bronchus. In the absence of palpable supraclavicular nodes, bronchoscopy is an inexpensive choice. Consistent with this, sufferers typically expertise a marked relief of signs and enchancment in high quality of life with chemotherapy. Occasionally patients fail to respond to chemoradiation, or expertise a relapse, but have resectable tumors. There are compelling, albeit restricted, knowledge suggesting that a considerable variety of these select patients may be cured by resection. Systematic review evaluating the timing of thoracic radiation remedy in combined modality remedy for limited-stage small-cell lung cancer. Diagnosis and remedy of lung cancer: an evidence-based guide for the practicing clinician. A prospective randomized trial to decide the benefit of surgical resection of residual illness following response of small cell lung most cancers to combination chemotherapy. She works in an workplace and smoked one to two packs of cigarettes per day until 5 years ago. Physical examination is unremarkable, together with range of motion of her left shoulder and chest auscultation. Differential Diagnosis this affected person has a classic presentation of a Pancoast tumor, with pain radiating down the arm and a refined, simply missed, abnormality on a chest radiograph. Often, numerous physicians deal with sufferers with such presentations for many months before the potential of a course of arising from the chest is entertained. A Pancoast tumor is a lung most cancers arising within the apex of the lung and involving constructions of the apical chest wall. Patients might or might not have the classic Pancoast syndrome of ache, weakness, or numbness radiating down the arm because of brachial plexus involvement. Discussion As with all lung cancers, sufferers with a Pancoast tumor should first bear a cautious history and physical examination to search for indicators of distant metastases. Tumor involvement in enlarged mediastinal or supraclavicular nodes must even be confirmed by cytology or biopsy due to a high false-positive rate. Discussion Because of the peripheral location in the lung and chest wall involvement, Pancoast tumors often present before distant metastases have occurred. However, the placement of these tumors is troublesome to strategy surgically, and makes resection with a wide margin problematic. Therefore, the technique of preoperative remedy has appeal, with the rationale that resection with a limited margin could additionally be extra more probably to be curative after preoperative remedy. Although chemotherapy could have an effect on systemic occult micrometastases, the primary position is as a radiation sensitizer, making the preoperative local remedy simpler. N2 node involvement has been a poor prognostic issue, making these sufferers unsuitable for resection except, maybe, the mediastinum is downstaged by preoperative therapy. Traditionally, involvement of the subclavian vessels, or invasion of a vertebral body or the neural foramina, has been viewed as a contraindication to resection. However, newer surgical approaches have been developed that enable complete resection of Pancoast tumors involving these buildings. Referral to a middle with specialised experience ought to be strongly thought-about earlier than both labeling a affected person as unresectable or making an attempt a resection with out confidence that an entire resection may be achieved. The natural history of untreated patients with Pancoast tumors is an average survival of 10 to 14 months after diagnosis, with symptoms of severe ache. There is suspected involvement of the first and second ribs and the lower nerve roots of the brachial plexus. Approach the patient has a localized, resectable tumor with no evidence of mediastinal or distant metastases. A strategy of preoperative therapy adopted by resection is Case 10 39 the pulmonary hilum and posterior chest wall and nerve roots. However, publicity of more anterior or cephalad structures is poor till the tumor is mobilized, making it difficult to achieve unfavorable margins alongside the brachial plexus past the nerve roots or alongside the subclavian vessels. Several anterior approaches have been developed, and are useful for tumors involving the center or anterior compartments of the thoracic inlet, and maybe for many tumors involving the posterior compartment as well. The anterior approaches include the anterior transcervical-thoracic approach and the cervicothoracic transmanubrial incision, popularized by Dartevelle. A transsternal approach, involving an incision above the clavicle and both a median sternotomy or partial sternotomy with extension into the fourth intercostal house, permits glorious publicity of the brachial plexus, the subclavian vessels, and the vertebral bodies, as do the other anterior approaches. Exposure of the pulmonary hilum could be troublesome with the transcervicalthoracic strategy. Surgical Approach After preoperative chemoradiotherapy, a sternotomy was carried out with an incision over the left clavicle toward the left deltopectoral groove. The left inside jugular vein and the left inner mammary artery had been each divided to facilitate retraction of the clavicle and anterior chest wall away from the tumor. The tumor concerned the upper ribs and T1 and T2 nerve roots, but not the subclavian vessels, the carotid artery, or the brachial plexus. The first and second ribs have been disarticulated from the vertebral bodies and transverse processes and divided within the deltopectoral groove.
Di-Arginine Malate (L-Arginine). Medrol. - Male infertility, prevention of the common cold, migraine headache, decreased mental function in the elderly, improving athletic performance, breast cancer when used in combination with chemotherapy, wound healing, female sexual problems, sickle cell disease, improving healing of diabetic foot ulcers, and improving the immune system in people with head and neck cancer.
- Preventing inflammation of the digestive tract in premature infants.
- Dosing considerations for L-arginine.
- Chest pain associated with coronary artery disease (angina pectoris).
- Problems with erections of the penis (erectile dysfunction).
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96845
Buy discount medrol 4 mg lineNote the epithelioid cytology with densely eosinophilic cytoplasm and abundant pale blue myxoid matrix lyme arthritis diet discount medrol 16mg with visa. These tumors typically have large epithelioid cells with vesicular nuclei arthritis and sports generic medrol 4 mg fast delivery, outstanding nucleoli arthritis pain relief cvs buy 16mg medrol visa, and brisk mitotic exercise arthritis pain elbow medrol 16mg free shipping. It consists of variably cohesive sheets of polygonal cells with a rhabdoid morphology. Cytologically, they characteristic giant, eccentric vesicular nuclei with distinguished nucleoli and a glassy, eosinophilic cytoplasmic inclusion. Note the adverse tumor cell nuclei amidst the positive stromal and endothelial cell nuclei. Awareness of this morphology is necessary to keep away from confusion with quite lots of different small round blue cell tumors, such as Ewing sarcoma. There are alternating areas of cellularity, and foci of myxoid background change are obvious. Plaque-Like Intravascular Growth Myxoid and Hypocellular (Left) Some areas of intimal sarcoma are relatively hypocellular with hyperchromatic atypical spindle cells set in a myxoid background. The bizarre cells are sometimes significantly enlarged and present anaplastic nuclear configurations and intensely deranged mitotic figures. The stroma is mostly collagenous, but is commonly tough to recognize as a end result of the high cellularity of the tumor. This discovering is extra frequent following neoadjuvant therapy, but may be seen in untreated tumors as nicely. This infiltrate is usually gentle or inconspicuous, however in occasional cases it can be marked (shown). However, on this location, a dedifferentiated liposarcoma is much extra probably and should all the time be totally excluded first. These cells are often also a function of extraskeletal osteosarcoma, which should always be excluded. However, if the myxoid change is diffuse or exhibits extra typical features of myxofibrosarcoma, the latter prognosis is extra applicable. Note the hypocellular, microcystic and sclerotic stroma, further evidence of treatment effect. Most tumors have extensive areas of geographic necrosis and sheets of intently spaced small spherical blue cells as depicted on this low-power micrograph. Cytologic Features Myxoid Matrix (Left) Although often sparse, extracellular myxoid matrix is current in most tumors. It normally presents as a small space of pale blue, hyalinized or nice fibrillary materials. Gross Appearance Gross Appearance (Left) this gross specimen is from an inguinal delicate tissue metastasis from a main popliteal mass in a 40-year-old man. The cut surface depicts a bulky, white, fleshy delicate tissue tumor with geographic areas of hemorrhagic necrosis. Note the tan gelatinous area that correspond to extracellular myxoid matrix of the tumor. The tumor ulcerated the skin, invaded and destroyed the underling bones, and spread proximally throughout the forearm (not shown). It confirmed no histologic response to remedy, which is noted grossly by intensive white, fleshy viable tumor. Geographic Necrosis Necrosis (Left) this medium-power micrograph illustrates the interface between viable neoplasm and coagulation tumor necrosis. This picture depicts a mediumsized blood vessel surrounded by a cuff of viable spherical cells inside an area of necrosis. The green probe, which marks the centromere of chromosome 19, shows the traditional 2 homologs. Nuclei are usually small, elongated, and bland, but occasionally larger nuclei are evident. Schwann Cells Subtle Proliferation (Left) Schwann cell hamartoma may lack nodularity and seem to subtly infiltrate the lamina propria as small, elongated groups of eosinophilic spindle cells. Careful looking and chopping of deeper ranges often reveal no much less than one ganglion cell in a true ganglioneuroma. Schwann Cell Component Ganglion Cells (Left) In some circumstances of ganglioneuroma, the ganglion cells are fairly numerous and kind clusters and loose aggregates. Perineurioma Perineurioma (Left) Perineurioma often proliferates between and across the colonic crypts, splaying them aside. Many instances additionally characteristically present a concentric "onion pores and skin" sample of development across the crypts. Perineurioma 732 Benign Neural Gastrointestinal Polyps Mesenchymal Tumors of the Gastrointestinal Tract Nuclear Vacuoles Perineurial Markers (Left) the nuclei of perineurioma are sometimes small, irregular, and pale, and normally present conspicuous nuclear vacuoles or pseudoinclusions. They are unfavorable for S100 protein, serving to to distinguish them from Schwann cell hamartoma and ganglioneuroma. Peripheral lymphoid aggregates and focal calcifications may also be seen at low power. It often presents as a small nodule endoscopically and could additionally be simply missed on a superficial biopsy. Note the distinguished eosinophilia of the subepithelial region, indicating the presence of a granular cell tumor. Most Common Site All sites Small and huge intestines Small bowel Stomach Stomach Stomach Small bowel Small bowel Response to Imatinib Therapy Excellent Comment Deletions associated with worse consequence (versus insertions and substitutions) Limited except larger dosage Sunitinib exhibits efficacy in setting of is used imatinib resistance Partial Poor Variable Poor or resistant Poor or resistant Poor or resistant 7. Rare D842V (most widespread exon 18 mutation) results in whole imatinib resistance Most reply to imatinib Most observe indolent scientific course Better overall consequence three. Joensuu H: Risk stratification of patients diagnosed with gastrointestinal stromal tumor. These had been discovered incidentally in a resection performed for a separate gastric carcinoma. Note additionally the tasteless, uniform, elongated nuclei attribute of most low-grade spindled tumors. Not uncommonly, hyalinization seems to type septa dividing sheets and nests of spindled tumor cells and imparting a lobular look. As seen in this image, the tissue can appear to tear aside and is related to myxoedematous stroma and hemorrhage. Some may even present irregular shapes ("staghorn") much like solitary fibrous tumor. This morphology is also classically related to Ewing sarcoma and malignant peripheral nerve sheath tumor. Perivascular Sparing Unusual Pseudopapillary Appearance (Left) Perivascular cuffing or retention of tumor cells may also be seen in a nonnecrotic background, as depicted.
Medrol 4 mg lowest priceCryptosporidia 252 Cryptosporidia Small Intestine: Nonneoplastic Cryptosporidia Adenoma Mimicking Cryptosporidia (Left) this small bowel biopsy exhibits a carpet of organisms arthritis treatment mumbai purchase medrol 4 mg without a prescription. Electron Microscopy Cryptosporidia in Colon (Left) Electron micrograph reveals a cryptosporidial organism situated throughout the brush border of the small intestine arthritis gel buy cheap medrol 4 mg on line. Isospora Cyclospora (Left) High-power view of the small bowel exhibits 2 Isospora organisms arthritis in neck order 4mg medrol with visa. They are much bigger than cryptosporidia and have a parasitophorous vacuole round them arthritis in back of leg cheap medrol 16mg on line. These organisms remain throughout the cytoplasm of the cell and have a parasitophorous vacuole. Isospora Isospora (Left) this image exhibits surface epithelial disarray with quite a few parasites present in parasitophorous vacuoles. Navaneethan U et al: Isospora belli superinfection in a affected person with eosinophilic gastroenteritis-a diagnostic problem. There are dense blue staining organisms surrounded by a transparent house, which is typical of the organism Cyclospora. Cyclospora Cyclospora (Left) High-power view exhibits the macrogametocyte stage of Cyclospora. The organism stains well with hematoxylin and is surrounded by a clear house (parasitophorous vacuole). There are crescent-shaped merozoites, microgametocytes, and macrogametocytes on this single high-power subject. Note that the vacuoles containing clusters of organisms "cup" the apical surface of the nucleus. Microsporidia Spores Microsporidia Spores and Plasmodia (Left) Specimen consisting of a plastic-embedded thick section for electron microscopy exhibits spores, as properly as plasmodial types of Microsporidia. Xiang H et al: New evidence on the connection between Microsporidia and Fungi: a genome-wide evaluation by DarkHorse software. Nonnecrotizing Granuloma Acute Ileocolitis (Left) Note the edema and ecchymosis of the terminal ileum. Manookian P et al: An unusual case of Yersinia enterocolitica infection manifesting as perianal and colonic ulcers. Note lymphoid hyperplasia and submucosal granulomas with outstanding lymphoid cuffs and giant cells. Golan L et al: Mycobacterium avium paratuberculosis invades human smallintestinal goblet cells and elicits irritation. Nonnecrotizing Granuloma With Lymphocytic Cuff Acid-Fast Bacterial Stain (Left) this acid-fast micro organism stain with oil immersion reveals several acid-fast bacteria inside macrophages. Giouleme O et al: Intestinal tuberculosis: a diagnostic challenge-case report and review of the literature. There can also be marked crypt distortion resembling chronic inflammatory bowel disease. Strongyloides Causing Chronic Colitis Colonic Strongyloides (Left) Colon biopsy exhibits Strongyloides stercoralis within the glandular epithelium, with associated cryptitis and increased mononuclear cells within the lamina propria. Gastric Strongyloides Small Intestinal Strongyloides (Left) this gastric antral biopsy reveals Strongyloides stercoralis within the gastric epithelium with minimal inflammation. There is villous blunting and larvae inside crypts but no significant inflammation. Strongyloides With Intense Eosinophilia Strongyloides With Giant Cell Reaction (Left) this small bowel biopsy reveals Strongyloides stercoralis in small bowel glandular epithelium with a dense eosinophilic infiltrate within the epithelium and lamina propria. Note the combination of plasma cells, macrophages, and eosinophils jamming the lamina propria. These nuclei can mimic a small yeast-like Histoplasma if the organism is cut in cross part. This "bottom heavy" pattern is commonly seen in adenomas of the small bowel quite than the colon. Note the presence of a more complicated structure and desmoplastic stroma on the left. Small Bowel Carcinoma Resembles Colon Cancer Carcinoma Arising in Crohn Disease and Dysplasia (Left) this picture shows villiform high-grade dysplasia on the floor with invasive adenocarcinoma beneath. Ellis L et al: Carcinoid tumors of the gastrointestinal tract: developments in incidence in England since 1971. Chetty R: An overview of practical points in the diagnosis of gastroenteropancreatic neuroendocrine pathology. Shia J et al: Is nonsmall cell kind high-grade neuroendocrine carcinoma of the tubular gastrointestinal tract a distinct disease entity The fibrous stroma is characteristic of carcinoid tumors and sometimes leads to kinking and obstruction of the bowel wall. Bland Homogeneous Cells Homogeneous Bland Cells (Left) High-power view exhibits a homogeneous nest of bland cells with plentiful pink cytoplasm typical of low-grade tumors. Chromogranin-A Stain Ki-67 Stain (Left) Chromogranin-A reveals diffuse granular staining in tumor cells, typical of a welldifferentiated neuroendocrine tumor. It is important to rely the area with probably the most positivity as this correlates best with prognosis. Somatostatinoma Somatostatin Stain (Left) Somatostatin stain reveals diffuse cytoplasmic staining in tumor cells of the duodenal somatostatinoma depicted in the identical case. Synaptophysin Stain Duct-Like Architecture (Left) Low-grade neuroendocrine tumor has a duct- or gland-like architecture, which might be misinterpreted as an adenocarcinoma. Trabecular Pattern 282 Well-Differentiated Neuroendocrine Tumor (Carcinoid), Small Intestine Small Intestine: Neoplastic Angiolymphatic Invasion Lymph Node Metastasis (Left) High-power view exhibits nests of low-grade tumor cells within the lamina propria. Note the bland appearance of the tumor cells although this is a metastasis. Neuroendocrine Carcinoma Synaptophysin Stain (Left) High-power view exhibits a high-grade neuroendocrine carcinoma. Chromogranin-A Stain Small Cell Carcinoma (Left) Chromogranin-A stain shows patchy staining in the identical poorly differentiated neuroendocrine carcinoma. This tumor has generic options seen in any small cell carcinoma ("salt and pepper" chromatin, nuclear molding, high mitotic count). The neoplasm is centered within the submucosa however most likely can be detectable on a mucosal biopsy. Gangliocytic Paraganglioma, Polypectomy Gangliocytic Paraganglioma (Left) this gangliocytic paraganglioma is centered within the submucosa but has focally extended via the muscularis mucosae to contain the mucosa. Even at low magnification, a spindle cell component and more epithelioid zones are obvious. An immunohistochemical and ultrastructural examine and a hypothesis concerning its origin. Gangliocytic Paraganglioma Gangliocytic Paraganglioma With Ampullary Glands (Left) this gangliocytic paraganglioma entails the ampullary area. The lesion is triphasic, with spindled schwannian, ganglion, and endocrine-type cells. Gangliocytic Paraganglioma Gangliocytic Paraganglioma, Ganglion Cell (Left) High-magnification picture shows a lesional ganglion cell. Gangliocytic Paraganglioma 286 Gangliocytic Paraganglioma Small Intestine: Neoplastic Gangliocytic Paraganglioma, Epithelioid Cells Gangliocytic Paraganglioma, Subtle Example (Left) Oil immersion picture exhibits excessive magnification of the epithelioid element of this gangliocytic paraganglioma. Gangliocytic Paraganglioma Mimicking Neuroendocrine Tumor Gangliocytic Paraganglioma (Left) this gangliocytic paraganglioma seems just like a well-differentiated neuroendocrine (carcinoid) tumor on this crushed mucosal biopsy.
Buy generic medrol 4mg on-lineLiegl B et al: Rhabdomyosarcomatous differentiation in gastrointestinal stromal tumors after tyrosine kinase inhibitor therapy: a novel type of tumor progression remedies for arthritis pain in joints generic medrol 16 mg on line. Miettinen M et al: Gastrointestinal stromal tumors in sufferers with neurofibromatosis 1: a clinicopathologic and molecular genetic research of forty five cases arthritis underarm pain order medrol 4mg without prescription. Miettinen M et al: Gastrointestinal stromal tumors of the jejunum and ileum: a clinicopathologic enteropathic arthritis definition purchase medrol 16mg mastercard, immunohistochemical arthritis in back of leg generic 16mg medrol visa, and molecular genetic examine of 906 circumstances earlier than imatinib with long-term follow-up. Miettinen M et al: Gastrointestinal stromal tumors: review on morphology, molecular pathology, prognosis, and differential prognosis. Miettinen M et al: Gastrointestinal stromal tumors of the stomach in youngsters and young adults: a clinicopathologic, immunohistochemical, and molecular genetic study of forty four circumstances with long-term follow-up and evaluation of the literature. Miettinen M et al: Gastrointestinal stromal tumors of the stomach: a clinicopathologic, immunohistochemical, and molecular genetic examine of 1765 cases with long-term follow-up. Tran T et al: the epidemiology of malignant gastrointestinal stromal tumors: an analysis of 1,458 circumstances from 1992 to 2000. Hirota S et al: Gain-of-function mutations of c-kit in human gastrointestinal stromal tumors. This characteristic is answerable for lesional hemorrhage when these tumors are treated with targeted remedy. The lesional cells are very uniform, a characteristic of mesenchymal tumors associated with attribute mutations. The lesion has prolonged into the submucosa, and the overlying mucosa seems inflamed. There is a chondroid background, and the tumor cells have quite a few cytoplasmic vacuoles. Cases corresponding to this must be addressed as diagnoses of exclusion with an appropriate immunolabeling panel. The bulk of the tumor is in the muscularis propria, however the lesion has extended into the submucosa and was recognized by mucosal biopsy. This plexiform pattern is characterized by nodules of neoplasm separated by muscularis propria in this case. Despite this discovering and many recurrences of her neoplasm, the patient has lived many years. The epicenter of the mass is within the mesentery, but it has infiltrated into the muscularis propria as well. Note the sweeping fascicular association of cells and the uniform collagen deposition. Mesenteric Fibromatosis Mesenteric Fibromatosis, High Magnification (Left) this high-power image shows a fibromatosis adjacent to a small vessel. Note that, in comparison with the vessels in a fibromatosis, the vessels listed right here are inconspicuous. Gastrointestinal Stromal Tumor 650 Mesenteric Fibromatosis Multiple Organs: Neoplastic Calcifying Fibrous Pseudotumor Calcifying Fibrous Pseudotumor (Left) this image reveals a calcifying fibrous pseudotumor. Mesenteritis Ossificans Mesenteritis Ossificans (Left) this picture reveals an example of mesenteritis ossificans (described as mesenteric heterotopic myositis ossificans). This presented in a patient with Crohn illness and was presumably initiated by transmural inflammation. Vascular "Onion Skinning" Vascular "Onion Skinning" (Left) this high-magnification picture exhibits the lesional cells of an inflammatory fibroid polyp. The nuclei are small (compare their size to the internal management eosinophils) and have smooth nuclear membranes and tiny nucleoli. This lesion appears looser and extra myxoid at scanning magnification than a gastric inflammatory fibroid polyp would. It lacks the whorled structure of gastric examples however shares the eosinophilic infiltrate. Inflammatory Fibroid Polyp, Colon Inflammatory Fibroid Polyp, Small Intestine (Left) this picture exhibits low magnification of a colonic inflammatory fibroid polyp. The outstanding lymphoid aggregates and vessels are akin to the features of gastric inflammatory fibroid polyp. It is centered within the submucosa but bulges into the lumen and in addition has prolonged a bit into the muscularis propria. Inflammatory Fibroid Polyp, Small Bowel Inflammatory Fibroid Polyp, Small Bowel (Left) Intussusception produced submucosal lesional edema. Certainly the gastrointestinal tract submucosa could be an uncommon web site for myxoid liposarcoma. The tumor cells are usually smaller than the endothelial cells, monotonous, and accompanied by plenty of eosinophils. Systemic Mastocytosis Producing Pseudopolyps 656 Inflammatory Fibroid Polyp Multiple Organs: Neoplastic Systemic Mastocytosis, Small Bowel Systemic Mastocytosis, Small Bowel (Left) Systemic mastocytosis is often subtle on histology. Note the world with what seems as clearing around each cell (so-called "fried egg" appearance). Systemic Mastocytosis, Small Intestine Systemic Mastocytosis (Left) At this magnification, neoplastic mast cells with oval nuclei (each surrounded by a halo) are readily obvious. Additionally eosinophils are quite distinguished, which is an overlapping feature with inflammatory fibroid polyp. Diagnosis of mastocytosis is subtle and requires contemplating it within the first place. Note the distinguished lymphoid cuff at the periphery of the neoplasm, which has its epicenter within the muscularis propria. Gastric Schwannoma Gastric Schwannoma (Left) that is an example of a gastric schwannoma with mild nuclear atypia. This lesion shaped a big mass that compressed 1 of the kidneys, but many such tumors are multilobulated. When the 2p23 breakpoint on chromosome 2 is rearranged (involved in a translocation), the orange and green alerts are separated and are visualized as distinct signals more than 1 sign width apart. The abnormal specimen thus has 1 fusion for the conventional chromosome 2, and 1 orange and 1 green sign for the rearranged chromosome 2 (1O1G1F). Inflammatory Myofibroblastic Tumor Inflammatory Myofibroblastic Tumor (Left) this inflammatory myofibroblastic tumor has extended from the small bowel mesentery into the lamina propria. Inflammatory Myofibroblastic Tumor Inflammatory Myofibroblastic Tumor, Myxoid Zone (Left) Note the free look of the stroma. Inflammatory Myofibroblastic Tumor, Myxoid Zone Inflammatory Myofibroblastic Tumor, Myxoid Zone (Left) this very highmagnification picture exhibits the outstanding nucleoli in the tumor cells to advantage. Epithelioid Inflammatory Myofibroblastic Sarcoma Epithelioid Inflammatory Myofibroblastic Sarcoma (Left) it is a recurrence from an ordinary-appearing inflammatory myofibroblastic tumor. It has aggressiveappearing features, epithelioid inflammatory myofibroblastic sarcoma. However, parasitic infections, lymphomas, and inflammatory cells near carcinomas can label with IgG4. Sclerosing Mesenteritis Sclerosing Mesenteritis (Left) this example of a tumefactive lesion lacked storiform fibrosis but has obliterative phlebitis and was not aware of steroids. Rosai-Dorfman Disease, Mesentery Rosai-Dorfman Disease, Mesentery (Left) that is the diagnostic zone.
References - Woener SJ, Abildgaard CF, French BN. Intracranial hemorrhage in children with idiopathic thrombocytopenic purpura. Pediarics. 1981;67:453-60.
- Sinha A, Avery P, Turner S, Bailey S, Cheetham T. Vitamin D status in pediatric patients with cancer. Pediatr Blood Cancer 2011;57:594-598.
- Ireland PE: Glands of the esophagus. Laryngoscope 43:351, 1933.
- Roche PJ, Hoare SA, Parker MG: A consensus DNA-binding site for the androgen receptor, Mol Endocrinol 6(12):2229n2235, 1992.
- Tjandra JJ, Fazio VW, Milsom JW, et al: Omission of temporary diversion in restorative proctocolectomyois it safe? Dis Colon Rectum 36:1007, 1993.
- Harris, S.J., Arambula-Cosio, F., Mei, Q. et al: The Probot - an active robot for prostate resection. Proc Inst Mech Eng H 1997;11:317-325.
|