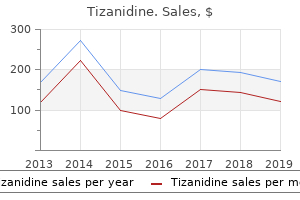
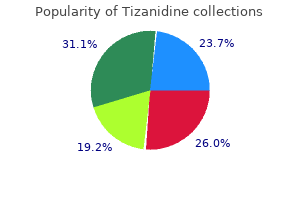
Tizanidine
Eva L. Feldman, M.D., Ph.D. - Department of Neurology
- University of Michigan
- Ann Arbor, MI
Cheap tizanidine 2mg onlineBursae are closed sacs ormed o serous membrane that occur in places topic to riction; they enable one structure to transfer reely over one other spasms thumb joint order tizanidine 4mg visa. Synovial tendon sheaths are longitudinal bursae that encompass tendons as they cross deep to retinacula or via fbrous digital sheaths muscle relaxant patch generic 2 mg tizanidine with visa. Bursal sacs enclose several constructions muscle relaxant menstrual cramps trusted tizanidine 4mg, similar to the heart muscle relaxant tinidazole discount tizanidine 4mg on-line, lungs, abdominal viscera, and tendons, very related to this collapsed balloon encloses the fst. A thin flm o lubricating uid between the parietal and visceral layers coners mobility to the structure surrounded by the bursa within a confned compartment. The transitional olds o synovial membrane between the continual parietal and visceral layers surrounding the connecting stalks (the wrist in this example) and/or neurovascular constructions serving the surrounded mass are known as mesenteries. The appendicular skeleton consists o the bones o the limbs, together with these orming the pectoral (shoulder) and pelvic girdles. Cartilage is a resilient, semirigid orm o connective tissue that orms parts o the skeleton the place extra fexibility is required-or example, the place the costal cartilages attach the ribs to the sternum. Also, the articulating suraces (bearing suraces) o bones collaborating in a synovial joint are capped with articular cartilage that provides smooth, low-riction, gliding suraces or ree motion. The proportion o bone and cartilage in the skeleton adjustments as the body grows; the younger a person is, the extra cartilage he or she has. Bone, a residing tissue, is a highly specialised, onerous orm o connective tissue that makes up most o the skeleton. A steady provide o new blood cells (produced by the marrow within the medullary cavity o many bones). A brous connective tissue masking surrounds each skeletal element like a sleeve, besides the place articular cartilage occurs; that surrounding bones is periosteum. The periosteum and perichondrium nourish the external aspects o the skeletal tissue. They are capable o laying down extra cartilage or bone (particularly during racture healing) and provide the interace or attachment o tendons and ligaments. They are distinguished by the relative quantity o solid matter and by the number and size o the spaces they include. All bones have a supercial skinny layer o compact bone around a central mass o spongy bone, except the place the latter is replaced by a medullary (marrow) cavity. Articular facets of vertebra Of rib: Head Neck Tubercle Body Spinous means of vertebrae Within the medullary cavity o adult bones, and between the spicules (trabeculae) o spongy bone, yellow (atty) or pink (blood cell and platelet orming) bone marrow-or a combination o both-is ound. The structure and proportion o compact and spongy bone differ according to unction. In lengthy bones designed or rigidity and attachment o muscles and ligaments, the amount o compact bone is greatest close to the middle o the shat the place the bones are liable to buckle. Right posterolateral view Humerus Capitulum Shaft Trochlea Greater trochanter of femur Ischial tuberosity Obturator foramen Classifcation o Bones Bones are classied based on their shape. Short bones are cuboidal and are ound only within the tarsus (ankle) and carpus (wrist). Other ormations relate to joints, the passage o tendons, and the availability o elevated leverage. Facet: smooth fats area, normally covered with cartilage, the place a bone articulates with one other bone. The mesenchymal cells condense and dierentiate into chondroblasts, dividing cells in rising cartilage tissue, thereby orming a cartilaginous bone model. In the midregion o the mannequin, the cartilage calcies (becomes impregnated with calcium salts), and periosteal capillaries (capillaries rom the brous sheath surrounding the model) grow into the calcied cartilage o the bone model and supply its interior. These blood vessels, together with related osteogenic (bone-orming) cells, orm a periosteal bud. The capillaries provoke the first ossifcation heart, so named because the bone tissue it orms replaces most o the cartilage in the principle body Epiphysial artery Periosteum Primary ossification center (diaphysis) Periosteal bud Cartilage 1 Secondary ossification middle (epiphysis) Epiphysial plate Diaphysis Epiphysial plate Metaphysis Nutrient artery (derived from periosteal bud) Secondary ossification middle (epiphysis) (A) Epiphysis Epiphysial plate Bone Development Most bones take a few years to grow and mature. All bones derive rom mesenchyme (embryonic connective tissue) by two dierent processes: intramembranous ossication (directly rom mesenchyme) and endochondral ossication (rom cartilage derived rom mesenchyme). The histology (microscopic structure) o a bone is identical by both course of (Pawlina, 2016). The two processes o bone improvement proceed as ollows: In intramembranous ossifcation (membranous bone ormation), mesenchymal models o bones orm in the course of the embryonic interval, and direct ossication o the mesenchyme begins in the etal period. In endochondral ossifcation (cartilaginous bone ormation), cartilage models o the bones orm rom mesenchyme in the course of the etal period, and bone subsequently replaces most o the cartilage. Growth in length happens on each side o the cartilaginous epiphysial plates (double-headed arrows). When development ceases, the depleted epiphysial plate is changed by a synostosis (bone-to-bone usion), noticed as an epiphysial line in radiographs and sectioned bone. The chondrocytes within the center o the epiphysis hypertrophy, and the bone matrix (extracellular substance) between them calcies. Epiphysial arteries grow into the creating cavities with related osteogenic cells. These development plates are finally replaced by bone at each o its two sides, diaphysial and epiphysial. The seam ormed during this usion process (synostosis) is particularly dense and is recognizable in sectioned bone or radiographs as an epiphysial line. Ossication o short bones is just like that o the primary ossication middle o long bones, and just one quick bone, the calcaneus (heel bone), develops a secondary ossication middle. The nutrient artery divides within the medullary cavity into longitudinal branches that proceed toward each finish, supplying the bone marrow, spongy bone, and deeper portions o the compact bone. However, many small branches rom the periosteal arteries o the periosteum are responsible or nourishment o most o the compact bone. Blood reaches the osteocytes (bone cells) within the compact bone by means o haversian systems or osteons (microscopic canal systems) that house small blood vessels. The ends o the bones are supplied by metaphyseal and epiphysial arteries that arise mainly rom the arteries that supply the joints. The periosteum is richly supplied with sensory nerves-periosteal nerves-that carry ache bers. The periosteum is particularly sensitive to tearing or rigidity, which explains the acute ache rom bone ractures. Within bones, vasomotor nerves cause constriction or dilation o blood vessels, regulating blood fow via the bone marrow. Many bones develop rom a number of facilities o ossication, and the separate elements normally use. Sometimes one o these centers ails to use with the principle bone, giving the appearance o an extra bone. Careul research reveals that the apparent further bone is a missing part o the primary bone. Circumscribed areas o bone are oten seen along the sutures o the cranium where the fat bones abut, Skeletal System 23 significantly these related to the parietal bone (see Chapter 8, Head). It is important to know that accessory bones are widespread in the oot, to avoid mistaking them or bone ragments in radiographs and other medical pictures. Ater several months, little proof o the racture remains, particularly in young individuals. Fractures are more frequent in children than in adults because o the combination o their slender, growing bones and careree activities.
Order 4mg tizanidine free shippingBoth nerve and artery break up into several branches that enter the deep surace o the overlying gluteus maximus muscle muscle relaxant education cheap tizanidine 4 mg fast delivery. It lies on the pelvic surace o the coccygeus and supplies this muscle spasms from anxiety buy discount tizanidine 2 mg line, part o the levator ani spasms hindi meaning order tizanidine 4mg amex, and the sacrococcygeal joint spasms right before falling asleep discount 4mg tizanidine with mastercard. The anococcygeal nerves arising rom this plexus pierce the coccygeus and anococcygeal ligament to provide a small area o skin between the tip o the coccyx and the anus. The superior hypogastric plexus is a continuation o the aortic plexus that divides into let and right hypogastric nerves as it enters the pelvis. The hypogastric and pelvic splanchnic nerves merge to orm the inerior hypogastric plexuses, which thereore consist o each sympathetic and parasympathetic fbers. Autonomic (sympathetic) fbers additionally enter the pelvis through the sympathetic trunks and peri-arterial plexuses. Neurovascular Structures o Pelvis 587 Peri-arterial plexuses: postsynaptic, sympathetic, vasomotor bers to superior rectal, ovarian, and inside iliac arteries and their derivative branches. Hypogastric plexuses: most necessary route by which sympathetic bers are conveyed to the pelvic viscera. Pelvic splanchnic nerves: pathway or parasympathetic innervation o pelvic viscera and descending and sigmoid colon. The sacral sympathetic trunks are the inerior continuation o the lumbar sympathetic trunks. Each o the sacral trunks is diminished in size rom that o the lumbar trunks and usually contains our sympathetic ganglia. The sacral trunks descend on the pelvic surace o the sacrum simply medial to the pelvic sacral oramina and converge to orm the small median ganglion impar (coccygeal ganglion) anterior to the coccyx. The sacral sympathetic trunks descend posterior to the rectum within the extraperitoneal connective tissue and ship speaking branches (gray rami communicantes) to each o the anterior rami o the sacral and coccygeal nerves. They additionally send small branches to the median sacral artery and the inerior hypogastric plexus. The main unction o the sacral sympathetic trunks is to present postsynaptic bers to the sacral plexus or sympathetic (vasomotor, pilomotor, and sudomotor) innervation o the decrease limb. The peri-arterial plexuses o the ovarian, superior rectal, and internal iliac arteries are minor routes by which sympathetic bers enter the pelvis. The hypogastric plexuses (superior and inerior) are networks o sympathetic and visceral aerent nerve bers. The main half o the superior hypogastric plexus is a prolongation o the intermesenteric plexus (see Chapter 2, Back), which lies inerior to the biurcation o the aorta. It carries bers conveyed to and rom the intermesenteric plexus by the L3 and L4 splanchnic nerves. The superior hypogastric plexus enters the pelvis, dividing into right and let hypogastric nerves, which descend on the anterior surace o the sacrum. These nerves descend lateral to the rectum within hypogastric sheaths and then spread in a an-like ashion as they merge with the pelvic splanchnic nerves to orm the proper and let inerior hypogastric plexuses. The inerior hypogastric plexuses thus comprise both sympathetic and parasympathetic bers in addition to visceral aerent bers, which proceed via the lamina o the hypogastric sheath to the pelvic viscera, upon which they orm subplexuses collectively reerred to as the pelvic plexuses. In both sexes, subplexuses are associated with the lateral elements o the rectum and inerolateral suraces o the bladder. In addition, subplexuses in the male are also related to the prostate and seminal glands. In emales, subplexuses are additionally associated with the cervix o the uterus and the lateral ornices o the vagina. Pelvic splanchnic nerves arise in the pelvis rom the anterior rami o spinal nerves S2�S4 o the sacral plexus. They convey presynaptic parasympathetic bers derived rom the S2�S4 spinal wire segments, which make up the sacral outfow o the parasympathetic (craniosacral) nervous system, and visceral aerent bers rom cell our bodies within the spinal ganglia o the corresponding spinal nerves. The hypogastric/pelvic system o plexuses, receiving sympathetic bers through lumbar splanchnic nerves and parasympathetic bers through pelvic splanchnic nerves, innervate the pelvic viscera. Although the sympathetic component largely produces vasomotion as elsewhere, here, it also inhibits peristaltic contraction o the rectum and stimulates contraction o the internal genital organs throughout orgasm, producing ejaculation within the male. The parasympathetic bers distributed throughout the pelvis stimulate contraction o the rectum and bladder or deecation and urination, respectively. Parasympathetic bers in the prostatic plexus penetrate the pelvic foor to attain the erectile our bodies o the external genitalia, producing erection. Thereore, in the case o the pelvis, they travel by way of the pelvic and inerior hypogastric plexuses and the pelvic splanchnic nerves to the spinal sensory ganglia o spinal nerves S2�S4. The paths ollowed by visceral aerent ibers conducting ache rom the pelvic viscera dier in phrases o course and vacation spot, relying on whether the viscus or half o the viscus rom which the pain is emanating is situated superior or inerior to the pelvic pain line. Except within the case o the alimentary canal, the pelvic ache line corresponds to the inerior restrict o the peritoneum (see Table 6. Intraperitoneal abdominopelvic viscera, or features o visceral structures which are in touch with the peritoneum, are superior to the pain line. Aerent bers conducting ache impulses rom the viscera or portions o viscera inerior to the ache line ollow the parasympathetic bers retrograde by way of the pelvic and inerior hypogastric plexuses and pelvic splanchnic nerves to attain cell bodies within the spinal sensory ganglia o S2�S4. As indicated in the description o the uterine artery, descriptions o the relationship o the artery to the ureter tend to be oversimplied as "passing superior to the ureter. The ureter is in peril o being inadvertently clamped (crushed), ligated, or transected during a hysterectomy (excision o uterus) when the uterine artery is ligated and severed to take away the uterus. The point at which the uterine artery and ureter cross lies roughly 2 cm superior to the ischial spine. Blood fow in the artery is maintained, though it may be reversed within the anastomotic branch. Injury to this nerve might cause painul spasms o the adductor muscular tissues o the thigh and sensory decits within the medial thigh region. Injury to the nerve to the levator ani, together with its branches to the pubococcygeus and/or puborectalis, as a result of stretching o the nerve throughout a vaginal birth, might lead to a loss o help o the pelvic viscera and urinary or ecal incontinence just like that ensuing rom tearing o the muscle. Abdominal aorta Stenotic phase of proper widespread iliac artery Left widespread iliac artery Median sacral artery Superior gluteal artery Internal iliac artery External iliac artery Femoral artery Obturator artery Ligation o Internal Iliac Artery and Collateral Circulation in Pelvis Occasionally, the inner iliac artery turns into stenotic (the lumen turns into narrow) as a outcome of atherosclerotic ldl cholesterol deposit. There is a site o narrowing (stenosis) o the best frequent iliac artery (circled area). Pelvic arteries: Multiple anastomosing arteries present a collateral circulatory system that helps guarantee an sufficient blood supply to the larger and lesser pelves. Most arterial blood is delivered to the lesser pelvis by the inner iliac arteries, which commonly biurcate into an anterior division (providing all the visceral branches) and a posterior division (usually completely parietal). Postnatally, the umbilical arteries become occluded distal to the origin o the superior vesical arteries and, in the male, the arteries to the ductus deerens. The inerior vesical (males) and uterine arteries (emales) provide the inerior bladder and pelvic urethra. The uterine artery is solely emale, but each sexes have middle rectal arteries.
Diseases - Bartter syndrome, antenatal form
- Axial mesodermal dysplasia
- EPP (erythropoietic protoporphyria)
- Congenital hepatic fibrosis
- Dislocation of the hip dysmorphism
- Keratosis palmoplantaris esophageal colon cancer
Tizanidine 2 mg fast deliveryIn addition to rmly tying the orearm bones collectively while permitting pronation and supination muscle relaxant high cheap 2 mg tizanidine with amex, the interosseous membrane supplies the proximal attachment or some deep orearm muscle tissue muscle relaxant skelaxin 800 mg discount 4mg tizanidine. The head o the ulna is at the distal finish o the orearm muscle relaxer kick in buy tizanidine 2mg, whereas the pinnacle o the radius is at its proximal end spasms between ribs buy tizanidine 2 mg low price. The function o orearm motion, occurring on the elbow and radioulnar joints, is to help the shoulder in the software o orce and in controlling the position o the hand in area. Compartments o Forearm As within the arm, the muscles o related purpose and innervation are grouped throughout the same ascial compartments within the orearm. Although the proximal boundary o the orearm per se is dened by the joint airplane o the elbow, unctionally the orearm includes the distal humerus. Furthermore, because the constructions on which the muscle tissue and tendons act (wrist and ngers) have an extensive range o movement, an extended vary o contraction is required, requiring that the muscular tissues have lengthy contractile parts in addition to an extended tendon(s). Generally, fexors lie anteriorly and extensors posteriorly; however, the anterior and posterior features o the distal humerus are occupied by the chie fexors and extensors o the elbow. To present the required attachment websites or the fexors and extensors o the wrist and ngers, medial and lateral extensions (epicondyles and supraepicondylar ridges) have developed rom the distal humerus. The medial epicondyle and supra-epicondylar ridge provide attachment or the orearm fexors, and the lateral ormations provide attachment or the orearm extensors. Thus, somewhat than mendacity strictly anteriorly and posteriorly, the proximal elements o the "anterior" (fexor�pronator) compartment o the orearm lie anteromedially, and the "posterior" (extensor�supinator) compartment lies posterolaterally. Spiraling progressively over the length o the orearm, the compartments become actually anterior and posterior in place in the distal orearm and wrist. These ascial compartments, containing the muscular tissues in unctional groups, are demarcated by the subcutaneous border o the ulna posteriorly (in the proximal orearm) after which medially (distal orearm) and by the radial artery anteriorly after which laterally. These constructions are palpable (the artery by its pulsations) all through the orearm. Because neither boundary is crossed by motor nerves, they also present websites or surgical incision. The exors and pronators o the orearm are within the anterior compartment and are served mainly by the median nerve; the one and a hal exceptions are innervated by the ulnar nerve. The extensors and supinators o the orearm are within the posterior compartment and are all served by the radial nerve (directly or by its deep branch). The anterior compartment is outstanding on this regard because it communicates with the central compartment o the palm through the carpal tunnel. In the proximal part o the orearm, the muscle tissue orm feshy masses extending ineriorly rom the medial and lateral epicondyles o the humerus. The tendons o these muscular tissues move via the distal part o the orearm and proceed into the wrist, hand, and ngers. The fexor muscle tissue o the anterior compartment have approximately twice the majority and strength o the extensor muscles o the posterior compartment. The tendons o most fexor muscle tissue are positioned on the anterior surace o the wrist and are held in place by the palmar carpal ligament and the fexor retinaculum (transverse carpal ligament), thickenings o the antebrachial ascia. A superfcial layer or group o our muscles (pronator teres, fexor carpi radialis, palmaris longus, and fexor carpi ulnaris). These muscles are all hooked up proximally by a typical fexor tendon to the medial epicondyle o the humerus, the widespread fexor attachment. A deep layer or group o three muscle tissue (fexor digitorum proundus, fexor pollicis longus, and pronator quadratus). Dissection displaying the superfcial muscular tissues o the orearm and the palmar aponeurosis. Cross sections demonstrating relationships at cubital ossa, proximal orearm, and wrist. At the level o the cubital ossa, the exors and extensor o the elbow occupy the anterior and posterior features o the humerus. Lateral and medial extensions (epicondyles and supraepicondylar ridges) o the humerus present proximal attachment (origin) or the orearm exors and extensors. Consequently, within the proximal orearm, the "anterior" exor�pronator compartment really lies anteromedially, and the "posterior" extensor�supinator compartment lies posterolaterally. The radial artery (laterally) and the sharp, subcutaneous posterior border o the ulna (medially) are palpable eatures separating the anterior and posterior compartments. No motor nerves cross both demarcation, making them useul or surgical approaches. At the extent o the wrist, 9 tendons rom three muscular tissues (and one nerve) o the anterior compartment o the orearm traverse the carpal tunnel; eight o the tendons share a standard synovial exor sheath. All muscular tissues in the anterior (fexor�pronator) compartment o the orearm are provided by the median and/or ulnar nerves (most by the median; just one and a hal exceptions are provided by the ulnar). Thereore, the brachioradialis is a serious exception to the rule that (1) the radial nerve provides only extensor muscles and (2) that all fexors lie within the anterior (fexor) compartment. The lengthy exors o the digits (fexor digitorum supercialis and fexor digitorum proundus) additionally fex the metacarpophalangeal and wrist joints. This action is reinorced by the fexor digitorum supercialis when speed and fexion against resistance are required. When the wrist is fexed at the identical time that the metacarpophalangeal and interphalangeal joints are fexed, the long fexor muscles o the ngers are operating over a shortened distance between attachments, and the motion resulting rom their contraction is consequently weaker. Extending the wrist will increase their operating distance, and thus, their contraction is extra ecient in producing a powerful grip. Tendons o the lengthy fexors o the digits cross via the distal part o the orearm, wrist, and palm and proceed to the medial our ngers. The fexor digitorum supercialis fexes the center phalanges, and the fexor digitorum proundus fexes the middle and distal phalanges. The ollowing discussion provides further particulars, starting with the muscles o the supercial and intermediate layers. The pronator teres, a usiorm muscle, is probably the most lateral o the supercial orearm fexors. I appearing usually, the muscle is distinguished and may be palpated at the medial margin o the cubital ossa. In the center o the orearm, its feshy belly is replaced by a protracted, fattened tendon that turns into cord-like because it approaches the wrist. To take a look at the fexor carpi radialis, the particular person is requested to fex the wrist in opposition to resistance. It has a short belly and a protracted, cord-like tendon that passes supercial to the fexor retinaculum and attaches to it and the apex o the palmar aponeurosis. The tendon lies deep and slightly medial to this nerve beore it passes deep to the fexor retinaculum. The ulnar nerve enters the orearm by passing between the humeral and ulnar heads o its proximal attachment.
Purchase 2mg tizanidine free shippingThe depressions lateral to the umbilical olds are the peritoneal ossae kidney spasms causes buy tizanidine 2 mg free shipping, each o which is a possible website or a hernia infantile spasms 9 month old proven tizanidine 4mg. The shallow ossae between the umbilical olds are as ollows: Supravesical ossae between the median and the medial umbilical olds muscle relaxant tinidazole discount 4 mg tizanidine, ormed because the peritoneum refects rom the anterior stomach wall onto the bladder spasms when falling asleep discount tizanidine 2 mg visa. The stage o the supravesical ossae rises and alls with lling and emptying o the bladder. Medial inguinal ossae between the medial and the lateral umbilical olds, areas additionally generally called inguinal triangles (Hesselbach triangles), that are potential sites or the less common direct inguinal hernias. Lateral inguinal ossae, lateral to the lateral umbilical olds, embody the deep inguinal rings and are potential websites or the most common type o hernia within the lower abdominal wall, the indirect inguinal hernia (see the Clinical Box "Inguinal Hernias," p. The supra-umbilical half o the internal surace o the anterior belly wall has a sagittally oriented peritoneal refection, the alciorm ligament, that extends between Aponeurosis of exterior oblique the superior anterior stomach wall and the liver. The spherical ligament is a brous remnant o the umbilical vein, which handed rom the umbilicus to the liver prenatally. Although the testis is located in the perineum postnatally, the male gonad initially orms within the abdomen. Its relocation out o the abdomen into the perineum through the inguinal canal accounts or many o the structural eatures o the area. The inguinal ligament is the thickened, underturned, inerior margin o the aponeurosis o the external indirect, orming a retinaculum that bridges the subinguinal space. A slit-like gap between the medial and the lateral crura o the exterior indirect aponeurosis, bridged by intercrural fbers, orms the superfcial inguinal ring. Anterolateral Abdominal Wall 425 the retinaculum spans the subinguinal area, by way of which move the fexors o the hip and neurovascular buildings serving a lot o the lower limb. These brous bands are the thickened inerolateral-most portions o the exterior oblique and aponeurosis and the inerior margin o the transversalis ascia. The inguinal ligament is a dense band constituting the ineriormost half o the external indirect aponeurosis. The most lateral o these bers continue to run along the pecten pubis because the pectineal ligament (o Cooper). Some o the extra superior bers an upward, bypassing the pubic tubercle and crossing the linea alba to mix with the decrease bers o the contralateral external oblique aponeurosis. The iliopubic tract is the thickened inerior margin o the transversalis ascia, which seems as a brous band working parallel and posterior (deep) to the inguinal ligament. The iliopubic tract, seen in the place o the inguinal ligament when the inguinal area is seen rom its internal (posterior) side. The inguinal ligament and iliopubic tract span and provide central power to an space o innate weak point within the physique wall in the inguinal area known as the myopectineal orifce (Fruchaud, 1956). This weak area, occurring in relation to constructions traversing the physique wall, is the positioning o direct and oblique inguinal and emoral hernias. It is the start o an evagination in the transversalis ascia that orms an opening like the doorway to a cave. Through this opening, the extraperitoneal ductus deerens (vas deerens) and testicular vessels in males (or round ligament o the uterus in emales) and genital department o the genitoemoral nerve cross to enter the inguinal canal. The transversalis ascia itsel continues into the canal, orming the innermost masking (internal ascia) o the buildings traversing the canal. The superfcial (external) inguinal ring is the exit by which the spermatic wire in males, or the spherical ligament in emales, and ilio-inguinal nerve emerge rom the inguinal canal. The supercial ring is a split that occurs within the diagonal, in any other case parallel bers o the external indirect aponeurosis just superolateral to the pubic tubercle. The elements o the aponeurosis that lie lateral and medial to , and orm the margins o, the supercial ring are crura (L. The lateral crus attaches to the pubic tubercle, and the medial crus attaches to the pubic crest. Fibers o the supercial layer o investing (deep) ascia overlying the external indirect muscle and aponeurosis, running perpendicular to the bers o the aponeurosis, cross rom one crus to the opposite throughout the superolateral part o the ring. The inguinal canal is generally collapsed anteroposteriorly towards the buildings it conveys. Between its two openings (rings), the inguinal canal has two walls (anterior and posterior), as nicely as a roo and foor. Posterior wall: ormed by the transversalis ascia; its medial half is reinorced by pubic attachments o the interior oblique and transversus abdominis aponeuroses that requently merge to variable extents into a common tendon-the inguinal alx (conjoint tendon)-and the refected inguinal ligament. Roo: ormed laterally by the transversalis ascia, centrally by musculo-aponeurotic arches o the internal oblique and transversus abdominis, and medially by the medial crus o the external indirect aponeurosis. Floor: ormed laterally by the iliopubic tract, centrally by gutter ormed by the inolded inguinal ligament, and medially by the lacunar ligament. The inguinal canal in adults is an indirect passage, approximately four cm lengthy, directed ineromedially by way of the inerior part o the anterolateral stomach wall. The major occupant o the inguinal canal is the spermatic wire in males and the round ligament o the uterus in emales. These are unctionally and developmentally distinct constructions that occur in the identical location. The inguinal canal additionally contains blood and lymphatic vessels, the ilio-inguinal nerve, and the genital branch o the genitoemoral nerve (n. The layers o the belly wall and the coverings o the spermatic cord and testis derived rom them are proven. Sagittal part o the anterior belly wall and inguinal canal at the plane proven in (A). Most groin hernias in males pass superior to the iliopubic tract (inguinal hernias), whereas most move inerior to it in emales (emoral hernias). Because o its relative weak point, the myopectineal orice is overlaid with prosthetic mesh positioned in the extraperitoneal retro-inguinal house ("space o Bogros") in many hernia repairs. The testes develop within the extraperitoneal connective tissue in the superior lumbar area o the posterior abdominal wall. The male gubernaculum is a brous tract connecting the primordial testis to the anterolateral belly wall on the web site o the uture deep ring o the inguinal canal. A peritoneal diverticulum, the processus vaginalis, traverses the creating inguinal canal, carrying muscular and ascial layers o the anterolateral stomach wall beore it because it enters the primordial scrotum. The testis begins to pass via the inguinal canal in the course of the 28th week and takes roughly 3 days to traverse it. The stalk o the processus vaginalis usually degenerates; nonetheless, its distal saccular part orms the tunica vaginalis, the serous sheath o the testis and epididymis (Moore et al. The ovaries additionally develop in the superior lumbar region o the posterior abdominal wall and relocate to the lateral wall o the pelvis. The processus vaginalis o the peritoneum traverses the transversalis ascia at the website o the deep inguinal ring, orming the inguinal canal as within the male, and protrudes into the creating labium majus, which is the emale homologue o (part corresponding to) the scrotum. The emale gubernaculum, a brous twine connecting the ovary and primordial uterus to the creating labium majus, is represented postnatally by the ovarian ligament, between the ovary and uterus, and the spherical ligament o the uterus (L. Except or its most inerior part, which turns into a serous sac engulng the testis, the tunica vaginalis, the processus vaginalis obliterates by the 6th month o etal improvement.
Tizanidine: 4 mg, 2 mg
Order 4 mg tizanidine otcThis branch runs distally on the interosseous membrane with the anterior interosseous department o the ulnar artery spasms film tizanidine 2mg visa. However spasms with kidney stone splint cheap 4 mg tizanidine otc, its sensory and motor bers are distributed in the orearm by two separate branches muscle relaxant prescriptions generic tizanidine 4mg with visa, the supercial (sensory or cutaneous) and deep radial/posterior interosseous nerve (motor) spasms near belly button generic 4mg tizanidine amex. It divides into these terminal branches as it seems within the cubital ossa, anterior to the lateral epicondyle o the humerus, between the brachialis and brachioradialis. The posterior cutaneous nerve o the orearm arises rom the radial nerve within the posterior compartment o the arm, as it runs along the radial groove o the humerus. Thus, it reaches the orearm independent o the radial nerve, descending in the subcutaneous tissue o the posterior facet o the orearm to the wrist, supplying the skin. The supercial branch o the radial nerve can be a cutaneous nerve, however it provides rise to articular branches as nicely. In the orearm, the radial artery courses between the extensor and the exor muscle groups. Deep dissection o the distal half o the orearm and proximal part o the hand exhibiting the course o the arteries and nerves. The deep department o the radial nerve, ater it pierces the supinator, runs within the ascial plane between supercial and deep extensor muscular tissues in shut proximity to the posterior interosseous artery. It supplies motor innervation to all of the muscle tissue with feshy bellies positioned entirely in the posterior compartment o the orearm (distal to the lateral epicondyle o the humerus). The medial cutaneous nerve o the orearm (medial antebrachial cutaneous nerve) is an independent branch o the medial cord o the brachial plexus. With the posterior cutaneous nerve o the orearm rom the radial nerve, each supplying the realm o skin indicated by its name, these three nerves provide all of the cutaneous innervation o the orearm. Except or the supercial veins, which oten course independently in the subcutaneous tissue, these neurovascular buildings normally exist as parts o neurovascular bundles. These bundles are composed o arteries, veins (in the limbs, often in the orm o accompanying veins), and nerves as well as lymphatic vessels, which are often surrounded by a neurovascular sheath o varying density. Surace Anatomy o Forearm Three bony landmarks are easily palpated at the elbow: the medial and lateral epicondyles o the humerus and the olecranon o the ulna. Forearm 235 posterolaterally when the orearm is prolonged, the top o the radius could be palpated distal to the lateral epicondyle. The posterior border o the ulna is subcutaneous and may be palpated distally rom the olecranon alongside the whole length o the bone. This landmark demarcates the posteromedial boundary separating the fexor�pronator (anterior) and extensor�supinator (posterior) compartments o the orearm. The cubital ossa, the triangular hollow space on the anterior surace o the elbow, is bounded medially by the prominence ormed by the fexor�pronator group o muscles which would possibly be connected to the medial epicondyle. The black dot on the dorsum o the hand indicates the position o the medial epicondyle. The cubital ossa is bounded laterally by the prominence o the extensor�supinator group o muscles connected to the lateral epicondyle. The pulsations o the radial artery can be palpated all through the orearm because it runs its supercial course rom the cubital ossa to the wrist (anterior to the radial styloid process), demarcating the anterolateral boundary separating the fexor�pronator and extensor�supinator compartments o the orearm. The bigger radial styloid process could be easily palpated on the lateral side o the wrist when the hand is supinated, notably when the tendons overlaying it are relaxed. The radial styloid process is situated roughly 1 cm extra distal than the ulnar styloid process. This relationship o the styloid processes is necessary within the prognosis o sure accidents within the wrist region. Proximal to the radial styloid course of, the suraces o the radius are palpable or a ew centimeters. Pain is elt over the lateral epicondyle and radiates down the posterior surace o the orearm. Repeated orceul fexion and extension o the wrist strain the attachment o the frequent extensor tendon, producing infammation o the periosteum o the lateral epicondyle (lateral epicondylitis). Fracture o Olecranon Fracture o the olecranon, referred to as a "ractured elbow" by laypersons, is frequent as a result of the olecranon is subcutaneous and protrusive. The typical mechanism o harm is a all on the elbow mixed with sudden powerul contraction o the triceps brachii. The ractured olecranon is pulled away by the active and tonic contraction o the triceps. Because o the traction produced by the tonus o the triceps on the olecranon ragment, pinning is often required. Mallet or Baseball Finger Sudden severe pressure on a long extensor tendon may avulse half o its attachment to the phalanx. This deormity outcomes rom the distal interphalangeal joint all of a sudden being orced into excessive fexion (hyperfexion) when, or instance, a baseball is miscaught or a nger is jammed into the bottom pad. These actions avulse (tear away) the attachment o the tendon to the base o the distal phalanx. Synovial Cyst o Wrist Sometimes a nontender cystic swelling seems on the hand, mostly on the dorsum o the wrist. The trigger o the cyst is unknown, but it might outcome rom mucoid degeneration (Salter, 1999). Synovial cysts are near and oten communicate with the synovial sheaths on the dorsum o the wrist (purple in gure). A cystic swelling o the widespread fexor synovial sheath on the anterior aspect o the wrist can enlarge enough to produce compression o the median nerve by narrowing the carpal tunnel (carpal tunnel syndrome). This syndrome produces ache and paresthesia (partial numbness, burning, or prickling) within the sensory distribution o the median nerve and clumsiness o nger actions (see the scientific box "Carpal Tunnel Syndrome"). High Division o Brachial Artery Sometimes the brachial artery divides at a more proximal stage than ordinary. In this case, the ulnar and radial arteries start in the superior or middle half o the arm, and the median nerve passes between them. Deep fascia of arm Superfcial Ulnar Artery In roughly 3% o people, the ulnar artery descends supericial to the lexor muscle tissue. This variation have to be saved in thoughts when perorming venesections or withdrawing blood or making intravenous injections. I an aberrant ulnar artery is mistaken or a vein, it could be damaged and produce bleeding. Variations in Origin o Radial Artery the origin o the radial artery could also be more proximal than ordinary; it may be a department o the axillary or brachial arteries. Flexion o the distal interphalangeal joints o the 2nd and 3rd digits is also misplaced. The capacity to fex the metacarpophalangeal joints o the 2nd and 3rd digits is aected as a outcome of the digital branches o the median nerve provide the first and 2nd lumbricals. Thus, when the individual attempts to make a st, the 2nd and third ngers remain partially extended ("hand o benediction").
2 mg tizanidine fast deliveryAutonomic nerves are primarily dropped at muscle relaxant jaw cheap tizanidine 4 mg overnight delivery the pelvis through the superior hypogastric plexus (sympathetic fbers) and pelvic splanchnic nerves (parasympathetic fbers) spasms in lower left abdomen buy tizanidine 2 mg without a prescription, the 2 merging to orm the inerior hypogastric and pelvic plexuses muscle relaxant non-prescription order tizanidine 2mg free shipping. Sympathetic fbers to the pelvis produce vasomotion and contraction o inner genital organs during orgasm; they also inhibit rectal peristalsis back spasms 38 weeks pregnant generic tizanidine 4mg free shipping. Pelvic parasympathetic fbers stimulate bladder and rectal emptying and extend to the erectile bodies o the exterior genitalia to produce erection. Visceral aerent fbers conducting ache rom constructions superior to the pelvic pain line (structures involved with the peritoneum, besides or the distal sigmoid colon and rectum) ollow the sympathetic fbers retrogradely to inerior thoracic and superior lumbar spinal ganglia. The bladder and rectum-true pelvic viscera-are inerior continuations o techniques encountered within the stomach. Except or eatures associated to sharing o the male urethra by the urinary and reproductive tracts, and physical relationships to the respective reproductive organs, there are comparatively ew distinctions between the male and emale pelvic urinary and gastrointestinal organs. The arrows point out transient narrowing o the lumina o the ureters resulting rom peristaltic contraction. The ureters are retroperitoneal; their superior abdominal parts are described in Chapter 5, Abdomen. As the ureters cross the biurcation o the common iliac artery (or the beginning o the exterior iliac artery), they cross over the pelvic brim, thus leaving the abdomen and entering the lesser pelvis. The pelvic elements o the ureters run on the lateral walls o the pelvis, parallel to the anterior margin o the higher sciatic notch, between the parietal pelvic peritoneum and the interior iliac arteries. Opposite the ischial backbone, they curve anteromedially, superior to the levator ani, and enter the urinary bladder. The ureters move obliquely by way of the muscular wall o the urinary bladder in an ineromedial path, getting into the outer surace o the bladder roughly 5 cm apart, but their internal openings into the lumen o the empty bladder are separated by only hal that distance. This indirect passage by way of the bladder wall orms a one-way "fap valve," the internal stress o the lling bladder inflicting the intramural passage to collapse. In addition, contractions o the bladder musculature act as a sphincter preventing the refux o urine into the ureters when the bladder contracts, growing inner stress throughout micturition. Urine passes down the ureters by means o peristaltic contractions, a ew drops being transported at intervals o 12�20 seconds. In males, the one structure that passes between the ureter and the peritoneum is the ductus deerens. The ureter lies posterolateral to the ductus deerens and enters the posterosuperior angle o the bladder, just superior to the seminal gland. It then passes close to the lateral half o the ornix o the vagina and enters the posterosuperior angle o the bladder. The arterial provide to the pelvic elements o the ureters is variable, with ureteric branches extending rom the frequent iliac, internal iliac, and ovarian arteries. The ureteric branches anastomose along the length o the ureter orming a continuous blood supply, although not necessarily eective collateral pathways. The most fixed arteries supplying the terminal elements o the ureter in emales are branches o the uterine arteries. The blood supply o the ureters is a matter o great concern to surgeons operating in the region (see the Clinical Box "Iatrogenic Compromise o Ureteric Blood Supply"). The venous drainage rom the pelvic parts o the ureters usually parallels the arterial provide, draining to veins with corresponding names. The nerves to the ureters derive rom adjoining autonomic plexuses (renal, aortic, superior, and inerior hypogastric;. Aerent (pain) bers rom the ureters ollow sympathetic bers in a retrograde course to reach the spinal ganglia and spinal wire segments o T10�L2 or L3. Branches supplying the stomach hal o the ureter strategy medially, whereas these supplying the pelvic hal method laterally. I essential, traction o the ureters is applied gently and solely towards the blood provide to avoid disruption o the small branches. Nerve fbers rom the renal, aortic, and superior and inerior hypogastric plexuses prolong to the ureter, carrying visceral aerent and sympathetic fbers to the T10�L2(3) spinal sensory ganglia and cord segments. Parasympathetic fbers, rom the S2�S4 spinal cord segments, are distributed to the pelvic part o the ureter. The bladder is a temporary reservoir or urine and varies in size, form, place, and relationships in accordance with its content material and the state o neighboring viscera. When empty, the adult urinary bladder is positioned within the lesser pelvis, lying partially superior to and partially posterior to the pubic bones. It is separated rom these bones by the potential retropubic space (o Retzius) and lies mostly inerior to the peritoneum, resting on the pubic bones and pubic symphysis anteriorly and the prostate (males) or anterior wall o the vagina (emales) posteriorly. The bladder is comparatively ree inside the extraperitoneal subcutaneous atty tissue, except or its neck, which is held rmly by the lateral ligaments o bladder and the tendinous arch o the pelvic ascia-especially its anterior component, the puboprostatic ligament in males and the pubovesical ligament in emales (see also. In emales, because the posterior side o the bladder rests immediately upon the anterior wall o the vagina, the lateral attachment o the vagina to the tendinous arch o the pelvic ascia, the paracolpium, is an indirect but essential actor in supporting the urinary bladder. In inants and younger youngsters, the urinary bladder is almost completely in the abdomen even when empty. An empty bladder in adults lies virtually entirely in the lesser pelvis, its superior surace level with the superior margin o the pubic symphysis. As the bladder lls, it enters the larger pelvis as it ascends within the extraperitoneal atty tissue o the anterior belly wall. Compare its relation to the anterior stomach wall, pubic symphysis, and level o the supravesical ossa to that o the nondistended (empty) bladder partially B. In this emale pelvis, the uterus was sectioned in its own median aircraft and is depicted as if it coincided with the median aircraft o the physique, which is seldom the case. With the bladder empty, the traditional disposition o the uterus proven here-bent on itsel (anteexed) at the junction o the physique and cervix o the uterus and tipped anteriorly (anteverted)-causes its weight to be borne primarily by the bladder. Adult bladder and prostate demonstrating their pelvic location (inset) and the suraces o the bladder. Coronal part o urinary bladder and prostate in the airplane o the prostatic urethra. The apex o the bladder points toward the superior edge o the pubic symphysis when the bladder is empty. The undus o the bladder is reverse the apex, ormed by the somewhat convex posterior wall. The body o the bladder is the main portion o the bladder between the apex and the undus. On both sides, the pubic bones and ascia overlaying the levator ani and superior obturator internus muscle lie in contact with the inerolateral suraces o the bladder. Consequently, in males, the undus is separated rom the rectum centrally by solely the ascial rectovesical septum and laterally by the seminal glands and ampullae o the ductus deerentes. In emales, the undus is directly related to the superior anterior wall o the vagina. Toward the neck o the male bladder, the muscle bers orm the involuntary internal urethral sphincter. This sphincter contracts during ejaculation to stop retrograde ejaculation (ejaculatory refux) o semen into the bladder. In males, the muscle bers in the neck o the bladder are steady with the bromuscular tissue o the prostate, whereas in emales, these bers are steady with muscle bers within the wall o the urethra. The ureteric orifces and the interior urethral orice are at the angles o the trigone o the bladder.
Trubulus (Puncture Vine). Tizanidine. - Are there safety concerns?
- Chest pain (angina), atopic dermatitis (eczema), problems with erections, anemia, cancer, coughs, intestinal gas (flatulence), and other conditions.
- How does Tribulus work?
- What is Tribulus?
- Enhancing athletic performance.
- Are there any interactions with medications?
- Dosing considerations for Tribulus.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96088
Quality tizanidine 4mgThe coracoclavicular ligament is a strong pair o bands that unite the coracoid course of o the scapula to the clavicle spasms lower left abdomen cheap 2mg tizanidine with visa, anchoring the clavicle to the coracoid process spasms paraplegic buy tizanidine 2mg overnight delivery. The coracoclavicular ligament consists o two ligaments quinine spasms generic 4 mg tizanidine, the conoid and trapezoid ligaments spasms detoxification purchase 2 mg tizanidine free shipping, that are oten separated by a bursa related to the lateral finish o the subclavius muscle. Its broad attachment (base o the triangle) is to the conoid tubercle on the inerior surace o the clavicle. The almost horizontal trapezoid ligament is attached to the superior surace o the coracoid course of and extends laterally to the trapezoid line on the inerior surace o the clavicle. The massive, spherical humeral head articulates with the comparatively shallow glenoid cavity o the scapula. Superiorly, this half o the capsule encroaches on the basis o the coracoid course of in order that the brous layer o the capsule encloses the proximal attachment o the lengthy head o the biceps brachii to the supraglenoid tubercle o scapula within the joint. The joint capsule has two apertures: (1) an opening between the tubercles o the humerus or passage o the tendon o the lengthy head o the biceps brachii. The extent o the synovial membrane o the glenohumeral joint is demonstrated on this specimen in which the articular cavity has been injected with purple latex and the fbrous layer o the joint capsule has been removed. Lansdown, Proessor o Medical Imaging, University o Toronto, Toronto, Ontario, Canada. The inerior half o the joint capsule, the only part not reinorced by the rotator cu muscle tissue, is its weakest space. Here, the capsule is particularly lax and lies in olds when the arm is adducted; nonetheless, it turns into taut when the arm is kidnapped. The synovial membrane strains the inner surace o the brous layer o the capsule and refects rom it onto the glenoid labrum and the humerus, as ar as the articular margin o the top. The synovial membrane additionally orms a tubular sheath or the tendon o the long head o the biceps brachii, where it lies within the intertubercular sulcus o the humerus and passes into the joint cavity. Dissection o the glenohumeral joint by which the joint capsule was sectioned and the joint opened rom its posterior facet as i it had been a book. The anterior, inside surace demonstrates the glenohumeral ligaments, which have been incised to open the joint. The prime unction o these muscles and the musculotendinous rotator cu is to hold the comparatively giant head o the humerus in the a lot smaller and shallow glenoid cavity o the scapula. The glenohumeral ligaments are three brous bands, evident solely on the interior facet o the capsule, that reinorce the anterior part o the joint capsule. These ligaments radiate laterally and ineriorly rom the glenoid labrum at the supraglenoid tubercle o the scapula and mix distally with the brous layer o the capsule as it attaches to the anatomical neck o the humerus. The coracohumeral ligament is a robust broad band that passes rom the base o the coracoid process to the anterior side o the greater tubercle o the humerus. The transverse humeral ligament is a broad brous band that runs roughly obliquely rom the greater to the lesser tubercle o the humerus, bridging over the intertubercular sulcus. This ligament converts the groove right into a canal, which holds the synovial sheath and tendon o the biceps brachii in place throughout actions o the glenohumeral joint. The bones, articular suraces, joint capsule, cavity o the joints, and the subacromial bursa. Although shown on the external aspect o the joint capsule, the glenohumeral ligaments are literally a eature noticed rom the inner side o the joint (as in. These ligaments strengthen the anterior side o the capsule o the glenohumeral joint, and the coracohumeral ligament strengthens the capsule superiorly. A, acromion; C, clavicle; G, glenoid cavity; Gr, greater tubercle o humerus; H, head o humerus; N, surgical neck o humerus. Kucharczyk, Chair o Medical Imaging and Clinical Director o Tri-Hospital Resonance Centre, Toronto, Ontario, Canada. This osseoligamentous structure orms a protective arch that overlies the humeral head, stopping its superior displacement rom the glenoid cavity. The supraspinatus muscle passes under this arch and lies deep to the deltoid as its tendon blends with the joint capsule o the glenohumeral joint as half o the rotator cu. Movement o the supraspinatus tendon, passing to the greater tubercle o the humerus, is acilitated because it passes underneath the arch by the subacromial bursa. This reedom results rom the laxity o its joint capsule and the large size o the humeral head compared with the small dimension o the glenoid cavity. The glenohumeral joint allows movements round three axes and permits fexion�extension, abduction�adduction, rotation (medial and lateral) o the humerus, and circumduction. When the arm is abducted without rotation, out there articular surace is exhausted and the larger tubercle contacts the coraco-acromial arch, stopping urther abduction. I the arm is then laterally rotated 180�, the tubercles are rotated posteriorly and extra articular surace becomes obtainable to continue elevation. Stiening or xation o the joints o the pectoral girdle (ankylosis) ends in a way more restricted vary o movement, even i the glenohumeral joint is regular. The bursa protects the tendon where it passes inerior to the foundation o the coracoid process and over the neck o the scapula. It usually communicates with the cavity o the glenohumeral joint through a gap within the brous layer o the joint capsule. Thus, it acilitates motion o the supraspinatus tendon under the coraco-acromial arch and o the deltoid over the joint capsule o the glenohumeral joint and the larger tubercle o the humerus. The glenohumeral joint is equipped by the anterior and posterior circumfex humeral arteries and branches o the suprascapular artery. The bursae across the glenohumeral joint are o particular clinical significance as a end result of some o them communicate with the joint cavity. Consequently, opening a bursa may imply getting into the cavity o the glenohumeral joint. The spool-shaped trochlea and spheroidal capitulum o the humerus articulate with the trochlear notch o the ulna and the marginally concave superior side o the pinnacle o the radius, respectively; thereore, there are humero-ulnar and humeroradial articulations. The articular suraces, coated with hyaline cartilage, are most ully congruent (in contact) when the orearm is in a position midway between pronation and supination and is fexed to a right angle. The skinny anterior aspect o the joint capsule has been eliminated to reveal the articulating suraces o the bones inside. The fbrous layer and synovial membrane o the joint capsule, the subtendinous and subcutaneous olecranon bursae, and humero-ulnar articulation o the elbow joint. The synovial membrane lines the inner surace o the brous layer o the capsule and the intracapsular nonarticular components o the humerus. It is also continuous ineriorly with the synovial membrane o the proximal radio-ulnar joint. The lateral, an-like radial collateral ligament extends rom the lateral epicondyle o the humerus and blends distally with the anular ligament o the radius, which encircles and holds the head o the radius in the radial notch o the ulna, orming the proximal radio-ulnar joint and allowing pronation and supination o the orearm. The medial, triangular ulnar collateral ligament extends rom the medial epicondyle o the humerus to the coronoid process and olecranon o the ulna and consists o three bands: (1) the anterior cord-like band is the strongest, (2) the posterior an-like band is the weakest, and (3) the slender oblique band deepens the socket or the trochlea o the humerus. This angle is made by the axes o the arm and orearm when the elbow is ully prolonged. This is claimed to enable or clearance o the broader emale pelvis as the limbs swing throughout strolling; nevertheless, no signifcant dierence exists concerning the unction o the elbow. The an-like radial collateral ligament is hooked up to the anular ligament o the radius, however its superfcial fbers proceed on to the ulna. The ulnar collateral ligament has a robust, spherical, cord-like anterior band (part), which is taut when the elbow joint is extended, and a weak, an-like posterior band, which is taut when the joint is exed.
Purchase tizanidine 4mgAter dilation o the vessel zanaflex muscle relaxant buy tizanidine 4mg with amex, an intravascular stent could also be introduced to keep the dilation muscle relaxant end of life 2 mg tizanidine free shipping. Intravascular stents are composed o rigid or semirigid tubular meshes spasms perineum buy tizanidine 2 mg fast delivery, collapsed throughout introduction muscle relaxant antidote discount tizanidine 2 mg with mastercard. Once in place, they increase or are expanded with a balloon catheter, to keep luminal patency. Coronary Bypass Grat Patients with obstruction o their coronary circulation and severe angina may endure a coronary bypass grat operation. The great saphenous vein is commonly harvested or coronary bypass surgery as a outcome of it (1) has a diameter equal to or greater than that o the coronary arteries, (2) could be easily dissected rom the lower limb, and (3) and oers relatively lengthy portions with a minimum incidence o valves or branching. A coronary bypass grat shunts blood rom the aorta to a stenotic coronary artery to enhance the fow distal to the obstruction. Revascularization o the myocardium may also be achieved by surgically anastomosing an internal thoracic artery with Collateral Circulation by way of the Smallest Cardiac Veins Reversal o fow in the anterior and smallest cardiac veins might bring luminal blood (blood rom the guts chambers) to the capillary beds o the myocardium in some areas, providing some further collateral circulation. Functional testing o the center includes exercise tolerance tests (treadmill stress tests), primarily to check the implications o possible coronary artery disease. Exercise tolerance checks are o considerable importance in detecting the cause o heartbeat irregularities. Balloon catheter headed toward coronary artery Coronary Occlusion and Conducting System o Heart Damage to the conducting system o the heart, oten ensuing rom ischemia caused by coronary artery illness, produces disturbances o cardiac muscle contraction. By making use of rm strain to the thorax over the inerior half o the sternal body (external or closed chest massage), the sternum moves posteriorly 4�5 cm. The increased intrathoracic pressure orces blood out o the guts into the great arteries. When the exterior stress is released and the intrathoracic stress alls, the heart once more lls with blood. I the center stops beating (cardiac arrest) during heart surgical procedure, the surgeon makes an attempt to restart it using inside or open-chest coronary heart therapeutic massage. Subendocardial branches Fibrillation o Heart Fibrillation is a number of, rapid, circuitous contractions or twitchings o muscular bers, together with cardiac muscle. In atrial brillation, the normal common rhythmical contractions o the atria are replaced by speedy irregular and uncoordinated twitchings o dierent components o the atrial partitions. The ventricles reply at irregular intervals to the dysrhythmic impulses received rom the atria, but usually, circulation remains satisactory. As a outcome, an irregular pattern o uncoordinated contractions happens within the ventricles, besides in these areas that are inarcted. Ventricular brillation is essentially the most disorganized o all dysrhythmias, and in its presence, no eective cardiac output occurs. Damage to one o the bundle branches leads to a bundlebranch block, in which excitation passes alongside the unaected department and causes a normally timed systole o that ventricle solely. In these instances, a cardiac pacemaker (articial coronary heart regulator) may be implanted to increase the ventricular rate o contraction to 70�80 per minute. Obviously, this vital half o the conducting system must be preserved during surgical repair o the deect. Defbrillation o Heart A debrillating electrical shock could additionally be given to the guts by way of the thoracic wall by way of giant electrodes (paddles). This shock causes cessation o all cardiac actions, and a ew seconds later, the center could begin to beat extra normally. As coordinated contractions and hence pumping o the center is re-established, a point o systemic (including coronary) circulation results. Here, the electrode is rmly xed to the trabeculae carneae within the ventricular wall and placed in touch with the endocardium. Cardiac Reerred Pain the center is insensitive to contact, cutting, cold, and warmth; nonetheless, ischemia and the buildup o metabolic products stimulate ache endings within the myocardium. The aerent pain bers run centrally in the middle and inerior cervical branches and especially within the thoracic cardiac branches o the sympathetic trunk. The axons o these main sensory neurons enter spinal cord segments T1 through T4 or T5, especially on the let facet. Cardiac reerred pain is a phenomenon whereby noxious stimuli originating within the heart are perceived by a person as ache arising rom a supercial half o the body-the skin on Viscera o Thoracic Cavity 381 the let upper limb, or example. Visceral reerred ache is transmitted by visceral aerent bers accompanying sympathetic bers and is usually reerred to somatic structures or areas such as a limb having aerent bers with cell bodies in the identical spinal ganglion and central processes that enter the spinal twine through the identical posterior roots (Natel, 2013). Anginal pain is usually elt as radiating rom the substernal and let pectoral areas to the let shoulder and the medial facet o the let upper limb. Oten, the lateral cutaneous branches o the 2nd and third intercostal nerves (the intercostobrachial nerves) join or overlap of their distribution with the medial cutaneous nerve o the arm. Consequently, cardiac ache is reerred to the higher limb as a outcome of the spinal wire segments o these cutaneous nerves (T1�T3) are also widespread to the visceral aerent terminations or the coronary arteries. Synaptic contacts may also be made with commissural (connector) neurons, which conduct impulses to neurons on the best aspect o comparable areas o the spinal twine. This occurrence explains why ache o cardiac origin, although normally reerred to the let side, may be reerred to the best side, each side, or the back. The heart is formed like a tipped-over pyramid, with the apex directed antero-ineriorly and to the let and the bottom opposite the apex (posterior). Each facet o the center includes a receiving chamber (atrium) and a suction�compression�expulsion chamber (ventricle). One-way semilunar valves (pulmonic and aortic) placed on the exit on both sides prevent backow (except that which flls the coronary arteries) and maintains the diastolic strain o the arteries. The chambers have a glistening endothelial lining, the endocardium; a muscular wall or myocardium, the thickness o which is proportional to the interior pressures occurring throughout the specifc chamber; and a glistening outer covering (the visceral layer o serous pericardium, or epicardium). The myocardium o the atria and ventricles (and the myogenic propagation o contracting stimuli by way of it) is connected to and separated by the connective tissue o the fbrous skeleton o the heart. The fbrous skeleton consists o our fbrous rings, two trigones, and the membranous elements o the cardiac septa. Only specialised muscle conducting contractile impulses rom the atria to the ventricles penetrates the fbrous skeleton at defned sites. The fbrous skeleton offers attachment or the myocardium and cusps o valves and maintains the integrity o the orifces. Coronary circulation: the circulatory system o the myocardium is unique in that the coronary arteries fll during ventricular diastole as a result o aortic recoil. The capillary beds o the myocardium drain primarily into the best atrium via veins emptying into the coronary sinus. However, the vein additionally may enter immediately into the chambers via the smallest cardiac veins. Occlusion o both coronary artery with subsequent inarction o nodal or conductive tissue could require placement o an artifcial cardiac pacemaker. Sympathetic stimulation produces vasodilation and parasympathetic stimulation produces vasoconstriction. Inerior continuation o the cervical viscera (trachea anteriorly and esophagus posteriorly) and associated nerves (let recurrent laryngeal nerve). To summarize systemically, the order o the major buildings in the superior mediastinum, rom anterior to posterior, is (1) thymus, (2) veins, (3) arteries, (4) airway, (5) alimentary tract, and (6) lymphatic trunks.
Generic 2 mg tizanidine mastercardPinching reers to compression o something between the thumb and index nger-or instance muscle relaxant commercial buy 4mg tizanidine otc, handling a teacup or holding a coin on edge muscle relaxant during pregnancy buy tizanidine 4 mg lowest price. The place o relaxation is assumed by an inactive hand- or example muscle relaxant 2265 generic 4 mg tizanidine free shipping, when the orearm and hand are laid on a desk muscle spasms youtube tizanidine 2mg low price. Fascia and Compartments o Palm the ascia o the palm is steady with the antebrachial ascia and the ascia o the dorsum o the hand. The palmar ascia is skinny over the thenar and hypothenar eminences, as thenar and hypothenar ascia, respectively. However, the palmar ascia is thick centrally where it orms the brous palmar aponeurosis and within the ngers the place it orms the digital sheaths. One uses the precision grip to maintain a coin to allow manipulation (D) and when pinching an object with fngertips (E). Casts or ractures are utilized most oten with the hand and wrist within the position o rest. When gripping an unattached rod loosely (G) or frmly (H), the 2nd and third carpometacarpal joints are inflexible and stable, however the 4th and fifth are saddle joints allowing exion and extension. The thin thenar and hypothenar ascia covers the intrinsic muscle tissue o the thenar and hypothenar eminences, respectively. Between the thenar and hypothenar muscle plenty, the central compartment o the palm is rooed by the thick palmar aponeurosis. Thenar fascia Fibrous digital sheath A medial fbrous septum extends deeply rom the medial border o the palmar aponeurosis to the 5th metacarpal. Medial to this septum is the medial or hypothenar compartment, containing the hypothenar muscles and bounded anteriorly by the hypothenar ascia. Similarly, a lateral fbrous septum extends deeply rom the lateral border o the palmar aponeurosis to the 3rd metacarpal. Lateral to this septum is the lateral or thenar compartment, containing the thenar muscle tissue and bounded anteriorly by the thenar ascia. Between the hypothenar and thenar compartments is the central compartment, bounded anteriorly by the palmar aponeurosis and containing the fexor tendons and their sheaths, the lumbricals, the supercial palmar arterial arch, and the digital vessels and nerves. The deepest muscular airplane o the palm is the adductor compartment containing the adductor pollicis. Between the fexor tendons and the ascia masking the deep palmar muscular tissues are two potential areas, the thenar area and the midpalmar area. The spaces are bounded by brous septa passing rom the perimeters o the palmar aponeurosis to the metacarpals. Between the 2 spaces is the especially robust lateral brous septum, which is attached to the 3rd metacarpal. Although most ascial compartments end on the joints, the midpalmar space is steady with the anterior compartment o the orearm through the carpal tunnel. Thenar muscular tissues within the thenar compartment: abductor pollicis brevis, fexor pollicis brevis, and opponens pollicis. Hypothenar muscle tissue in the hypothenar compartment: abductor digiti minimi, fexor digiti minimi brevis, and opponens digiti minimi. Short muscles o the hand, the lumbricals, in the central compartment with the lengthy fexor tendons. The proximal end or apex o the triangular palmar aponeurosis is steady with the fexor retinaculum and the palmaris longus tendon. When the palmaris longus is current, the palmar aponeurosis is the expanded tendon o the palmaris longus. Distal to the apex, the palmar aponeurosis orms our longitudinal digital bands or rays that radiate rom the apex and fasten distally to the bases o the proximal phalanges and become continuous with the brous digital sheaths. The excessive diploma o reedom o the movements results rom the first metacarpal being independent, with cell joints at both ends. Transverse part through the center o the palm illustrating the ascial compartments o the hand. The midpalmar house underlies the central compartment o the palm and is related distally to the synovial tendon sheaths o the 3rd�5th digits and proximally to the frequent exor sheath as it emerges rom the carpal tunnel. The thenar area underlies the thenar compartment and is related distally to the synovial tendon sheath o the index fnger and proximally to the frequent exor sheath distal to the carpal tunnel. This motion happens on the carpometacarpal joint and leads to a "cupping" o the palm. Bringing the tip o the thumb into contact with the fifth nger, or any o the other ngers, entails considerably more motion than could be produced by the opponens pollicis alone. The rst our movements o the thumb occur on the carpometacarpal and metacarpophalangeal joints. Opposition, a complex motion, begins with the thumb in the prolonged position and initially entails abduction and medial rotation o the 1st metacarpal (cupping the palm) produced by the motion o the opponens pollicis on the carpometacarpal joint and then fexion at the metacarpophalangeal joint. In pulp-to-pulp opposition, actions o the nger opposing the thumb are also involved. This can be confrmed by noting the course the nail o the thumb aces in contrast with the nails o the other fngers. Thus, abduction and adduction happen in a sagittal airplane and exion and extension occur in a coronal airplane. Opposition, the motion bringing the tip o the thumb in contact with the pulps o the other fngers. The elements o opposition are abduction and medial rotation on the carpometacarpal joint and exion o the metacarpophalangeal joint. The pores and skin and subcutaneous tissue have been eliminated, as have most o the palmar aponeurosis and the thenar and hypothenar asciae. The superfcial palmar arch is situated immediately deep to the palmar aponeurosis, superfcial to the lengthy exor tendons. Three thenar and three hypothenar muscular tissues connect to the exor retinaculum and to the our marginal carpal bones united by the retinaculum. It fexes and rotates the 1st metacarpal medially on the carpometacarpal joint throughout opposition; this motion happens when picking up an object. The an-shaped muscle has two heads o origin, that are separated by the radial artery as it enters the palm to orm the deep palmar arch. Deep dissection o the palm revealing the anastomosis o the palmar carpal department o the radial artery with the palmar carpal branch o the ulnar artery to orm the palmar carpal arch and deep palmar arch. The abductor digiti minimi is probably the most supercial o the three muscles orming the hypothenar eminence. The abductor digiti minimi abducts the 5th nger and helps fex its proximal phalanx. The exor digiti minimi brevis is variable in measurement; it lies lateral to the abductor digiti minimi. The fexor digiti minimi brevis fexes the proximal phalanx o the fifth nger on the metacarpophalangeal joint. The opponens digiti minimi is a quadrangular muscle that lies deep to the abductor and lexor muscular tissues o the 5th inger.
Purchase 4 mg tizanidine fast deliverySeveral parts o the gastrointestinal tract and associated organs become secondarily retroperitoneal spasms thumb joint order tizanidine 2mg without prescription. A mesentery connects an intraperitoneal organ to the physique wall-usually the posterior stomach wall muscle relaxant herniated disc generic 4 mg tizanidine. The small intestine mesentery is often reerred to simply as "the mesentery"; nonetheless muscle relaxant properties of xanax order tizanidine 2 mg amex, mesenteries related to different specic parts o the alimentary tract are named accordingly-or instance spasms around the heart tizanidine 4mg amex, the transverse and sigmoid mesocolons. Mesenteries have a core o connective tissue containing blood and lymphatic vessels, nerves, lymph nodes, and at. An omentum is a double-layered extension or old o peritoneum that passes rom the abdomen and proximal half o the duodenum to adjacent organs in the abdominal cavity. The higher omentum is a distinguished, our-layered peritoneal old that hangs down like an apron rom the greater curvature o the abdomen and the proximal part o the duodenum. Ater descending, it olds again and attaches to the anterior surace o the transverse colon and its mesentery. The lesser omentum is a much smaller, double-layered peritoneal old that connects the lesser curvature o the abdomen and the proximal part o the duodenum to the liver. It additionally connects the abdomen to a triad o constructions that run between the duodenum and liver within the ree edge o the lesser omentum. The hepatogastric and hepatoduodenal ligaments are continuous elements o the lesser omentum and are separated only or descriptive convenience. The stomach is related to the: inerior surace o the diaphragm by the gastrophrenic ligament. All these buildings have a continuous attachment along the larger curvature o the stomach and are all part o the larger omentum, separated only or descriptive purposes. Some o the acts relating to this include the ollowing: the peritoneal cavity homes an excellent size o gut, most o which is covered with peritoneum. Extensive continuities are required between the parietal and visceral peritoneum to convey the necessary neurovascular buildings rom the body wall to the viscera. Various terms are used to describe the components o the peritoneum that connect organs with other organs, or to the abdominal wall, and the compartments and recesses that are ormed as a consequence. A mesentery is a double layer o peritoneum that happens consequently o the invagination o the peritoneum by an organ and constitutes a continuity o the visceral and parietal peritoneum. In this opened peritoneal cavity, parts o the higher omentum, transverse colon, and the small gut and its mesentery have been reduce away to reveal deep buildings and the layers o the mesenteric constructions. The mesentery o the jejunum and ileum (small intestine) and sigmoid mesocolon have been reduce near their parietal attachments. The larger omentum is shown in its "regular" place, covering most o the stomach viscera. The lesser omentum, attaching the liver to the lesser curvature o the stomach, is shown by reecting the liver and gallbladder superiorly. The larger omentum has been removed rom the greater curvature o the abdomen and transverse colon to reveal the intestines. The greater omentum has been reected superiorly, and the small gut has been retracted to the best side to reveal the mesentery o the small gut and the transverse mesocolon. Such areas are known as naked areas, ormed in relation to the attachments o the peritoneal ormations to the organs, including mesenteries, omenta, and ligaments that convey the neurovascular structures. Some peritoneal olds contain blood vessels and bleed i cut, such as the lateral umbilical olds, which include the inerior epigastric arteries. The central half o the greater omentum has been minimize out to present its relation to the transverse colon and mesocolon. The time period higher omentum is oten used as a synonym or the gastrocolic ligament, nevertheless it actually additionally includes the gastrosplenic and gastrophrenic ligaments, all o which have a continuous attachment to the higher curvature o the stomach. The hepatoduodenal ligament (ree edge o lesser omentum) conveys the portal triad: hepatic artery, bile duct, and portal vein. Subdivisions o Peritoneal Cavity Ater the rotation and improvement o the higher curvature o the abdomen throughout growth (see the Clinical Box "Brie Review o Embryological Rotation o Midgut," p. A surgical incision via the anterolateral stomach wall enters the greater sac. The transverse mesocolon (mesentery o the transverse colon) divides the abdominal cavity into a supracolic compartment, containing the abdomen, liver, and spleen, and an inracolic compartment, containing the small intestine and ascending and descending colon. The inracolic compartment lies posterior to the greater omentum and is divided into proper and let inracolic spaces by the mesentery o the small gut. Free communication occurs between the supracolic and the inracolic compartments by way of the paracolic gutters, the grooves between the lateral side o the ascending or descending colon and the posterolateral stomach wall. The omental bursa is an intensive sac-like cavity that lies posterior to the stomach, lesser omentum, and adjacent constructions. The omental bursa has a superior recess, limited superiorly by the diaphragm and the posterior layers o the coronary ligament o the liver, and an inerior recess between the superior elements o the layers o the larger omentum. The omental bursa permits ree movement o the stomach on the buildings posterior and inerior to it as a end result of the anterior and posterior partitions o the omental bursa slide easily over one another. Most o the inerior recess o the bursa turns into sealed o rom the primary half posterior to the abdomen ater adhesion o the anterior and posterior layers o the higher omentum. The omental bursa communicates with the larger sac by way of the omental oramen (epiploic oramen), an opening situated posterior to the ree edge o the lesser omentum (hepatoduodenal ligament). This median section o the abdominopelvic cavity shows the subdivisions o the peritoneal cavity. The supracolic and inracolic compartments o the higher sac are shown ater elimination o the larger omentum. The inracolic spaces and paracolic gutters decide the ow o ascitic uid (arrows) when inclined or upright. The boundaries o the omental oramen are as ollows: Anteriorly: the hepatoduodenal ligament (ree edge o lesser omentum), containing the hepatic portal vein, hepatic artery, and bile duct. This part shows that the omental bursa is an isolated half o the peritoneal cavity, mendacity dorsal to the abdomen and lengthening superiorly to the liver and diaphragm (superior recess) and ineriorly between the layers o the higher omentum (inerior recess). The red arrows move rom the higher sac via the omental oramen into the omental bursa. The index fnger is passing rom the larger sac via the omental oramen into the omental bursa (lesser sac). The hepatoduodenal ligament is being pinched between thumb and index fnger, which might compress the buildings o the portal triad (portal vein, hepatic artery, and bile duct). A main mechanism in stopping such inection is a mucous plug that eectively blocks the external os (opening) o the uterus to most pathogens, however to not sperm cells. It is the covering o visceral peritoneum (oten reerred to clinically as the serosa) that makes watertight end-to-end anastomoses o intraperitoneal organs, such as the small gut, comparatively straightforward to obtain. It is extra dicult to obtain watertight anastomoses o extraperitoneal buildings which have an outer adventitial layer, such as the thoracic esophagus.
References - Amin MB, Crotty TB, Tickoo SK, et al: Renal oncocytoma: a reappraisal of morphologic features with clinicopathologic findings in 80 cases, Am J Surg Pathol 21(1):1n12, 1997.
- Arturson G. Capillary permeability in burned and nonburned areas in dogs. Acta Chir Scand. 1961;274:55-103.
- Le Fort R. Fractures de la machoire superieure. Rev Chir 1901; 4:360.
- Brennan JF 3rd, Romer TJ, Lees RS, et al: Determination of human coronary artery composition by Raman spectroscopy. Circulation 1997;96:99-105.
|